
Gastrointestinal disorders such as bleeding, varices, blockages, and organ-related issues often require precise and timely intervention. Dr. Ravi Manek performs minimally invasive, image-guided gastroenterology procedures that target the root cause with exceptional accuracy.
These treatments help control internal bleeding, manage portal hypertension, and treat conditions affecting the stomach, liver, spleen, and digestive tract—without the need for major surgery. Patients benefit from reduced complications, shorter hospital stays, and quicker return to normal life.
With advanced expertise in GI interventions, Dr. Manek ensures every patient receives safe, effective, and highly specialized care tailored to their digestive health needs.
Acute gastrointestinal bleeding (GIB) can lead to significant morbidity and mortality without appropriate treatment. Massive bleeding can cause hemodynamic instability, which leads to hemorrhagic shock and even death in some patients with serious conditions
There are numerous causes of acute GIB including infection, vascular anomalies, inflammatory diseases, trauma and malignancy.
The diagnostic and therapeutic approach of GIB depends on its location, severity, and etiology.
Computed tomography angiography is usually enough, rarely nuclear scintigraphy is done localize the source of bleeding and provide essential information for the interventional radiologist to guide therapeutic management.
For patients with abnormal angiography, embolisation is effective therapeutically.
The types of embolisation agents, specifications, and methods of embolisation vary depending on arteriographic manifestations, bleeding locations, causes of disease, blood coagulation state, etc.
Commonly used GI arterial hemorrhage embolic materials include gelatin sponges, PVA particles, coils, etc.
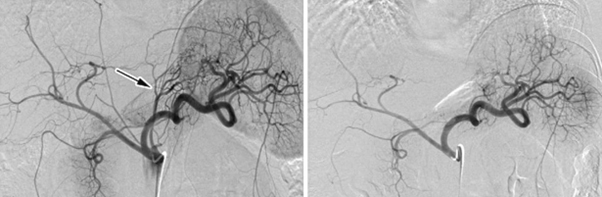
Acute mesenteric ischemia means bowel attack due to reduction or cessation of arterial inflow small intestinal, most commonly to the superior mesenteric artery (SMA).
Acute Ischemia due to acute mesenteric arterial occlusion caused by emboli. Chronic ischemia is usually due to atherosclerotic narrowing/occlusion of artery.
Patients may present with severe abdominal pain despite mild physical signs.
Endovascular therapy, including aspiration thrombectomy and local thrombolytic therapy, angioplasty and stent placement effective treatment option for mesenteric ischemia.
The key to endovascular treatment is to establish blood flow quickly before irreversible intestinal necrosis occurs.
Visceral is a collective term for an organ in your body, such as the liver or spleen, so a visceral aneurysm is an aneurysm that occurs in an organ. Abdominal visceral artery pseudoaneurysms are potentially lethal vascular lesions that arise from splanchnic circulation and the renal artery, as a result of various causes including inflammation, infection, trauma, and neoplasm. Unlike true aneurysms that have all three arterial wall layers, pseudoaneurysms develop due to disruption of intimal and medial layers of the arterial wall and do not contain any epithelized wall. They are outlined by thin fibrous tissue and usually surrounded by peri-arterial hematoma. The incidence of rupture and bleeding of pseudoaneurysms varies from 2% to 80% depending on the location, with untreated mortality rates reaching up to 100%. Due to the high risk of rupture and bleeding, treatment of these pseudoaneurysms is necessary.
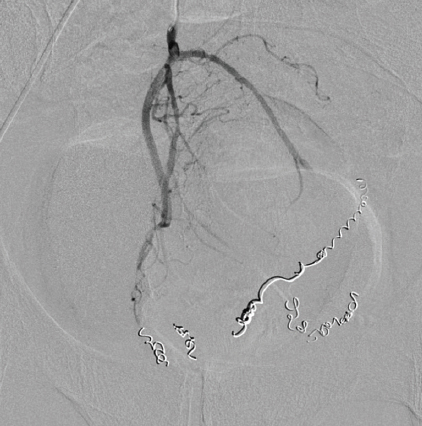
Pseudoaneurysm embolization is a minimally invasive procedure that involves transcatheter occlusion of the aneurysm/ artery and/or its branch vessels using metallic coils, PVA particles, Glue, or other embolic devices.
Splenic artery embolization (SAE) is an accepted nonsurgical intervention for the treatment of a variety of clinical disorders like splenic trauma, treatment of hypersplenism, blockage of splenic artery aneurysms or pseudoaneurysms, control of gastric variceal hemorrhage due to splenic vein thrombosis or portal hypertension and reduction of operative blood loss during splenectomy.
This minimally invasive procedure involves transcatheter occlusion of the splenic artery and/or its branch vessels using metallic coils, PVA particles, Glue, or other embolic devices.
One of the direct complications of chronic liver disease is Portal hypertension, which results in one of the life-threatening complications associated with the disease, in the form of gastric variceal bleeding.
Gastric variceal bleeding describes the bleeding that occurs when dilated vessels in the stomach rupture, and is associated with high morbidity and mortality rates. BRTO is a minimally invasive technique that involves blocking the dilated vessels, reducing the risk of rupture
Large portosystemic shunts at times can also cause symptoms of hepatic encephalopathy. these symptoms can also be alleviated by this procedure.
The procedure is performed under local anesthesia, via a femoral venous puncture, following which access is gained into the culprit shunt (most commonly being a splenorenal, flexible tube with a tiny balloon at one end) through a vein in your thigh or neck and guide the catheter to the liver using fluoroscopy for guidance. The catheter is then directed to the gastro renal or gastric aval shunt and the balloon is expanded to block the shunt.
The interventional radiologist will then perform venography, which is a type of imaging technique in which X-rays are used to see the vessels clearly. This will allow the interventional radiologist to confirm exactly which vessels need to be treated and if any other abnormal or dilated vessels have not previously been identified. Medication will then be injected into the dilated vessels through the catheter until they are completely filled. This medication will remain in the vessel for a short period, and will then be removed under fluoroscopy.
Another venography will then be performed, to confirm that the blood flow in the shunt has stopped. Finally, the balloon will be deflated and the interventional radiologist will withdraw the catheter.
One of the direst complications of chronic liver disease is Portal hypertension, which results in one of the life-threatening complications associated with the disease, in the form of gastric variceal bleeding.
Gastric variceal bleeding describes the bleeding that occurs when dilated vessels in the stomach rupture, and is associated with high morbidity and mortality rates. PARTO is a minimally invasive technique that involves blocking the dilated vessels, reducing the risk of rupture.
Large portosystemic shunts at times can also cause symptoms of hepatic encephalopathy. these symptoms can also be alleviated by this procedure.
The procedure is performed under local anesthesia, via a femoral venous puncture, following which access is gained into the culprit shunt (most commonly being a leinorenal, flexible tube with a tiny balloon at one end) through a vein in your thigh or neck and guide the catheter to the liver using fluoroscopy for guidance. The catheter is then directed to the gastro renal or gastric aval shunt and the plug device is expanded to block the shunt.
The interventional radiologist will then perform venography, which is a type of imaging technique in which X-rays are used to see the vessels clearly. This will allow the interventional radiologist to confirm exactly which vessels need to be treated and if any other abnormal or dilated vessels have not previously been identified. Medication will then be injected into the dilated vessels through the catheter until they are completely filled. This medication will remain in the vessel for a short period, and will then be removed under fluoroscopy.
Another venography will then be performed, to confirm that the blood flow in the shunt has stopped. Finally, the interventional radiologist will withdraw the catheter.
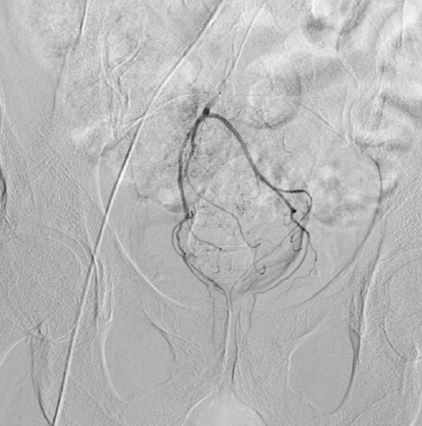
Hemorrhoids are a common anorectal disease that affects millions of people worldwide and are a major medical and socioeconomic problem. Internal hemorrhoids are composed of a dense anastomotic arteriovenous network, the corpus cavernosum recti (CCR). The CCR is dependent on the influx of arterial blood from the branches of the inferior mesenteric artery (the superior rectal arteries (Figure 1 and Figure 2). The lower part of the rectum and the anal canal are supplied with blood by the inferior and middle rectal arteries, both of which have origins from the internal iliac artery.
The replacement of muscle tissue with connective tissue causes an expansion of this vascular network of the anorectal submucosa, initiating a negative vicious cycle of progressive vascular dilation and venous insufficiency leading to hemorrhoidal hyperplasia, which in turn causes an increase in arterial inflow in the CCR and leads to symptoms.
Chronic bleeding is the primary symptom of internal hemorrhoids and could be associated with hemorrhoidal prolapse. It is widely accepted that it is difficult for patients to assess bleeding themselves, and assessment is even more difficult in this context, due to the intermittent nature of hemorrhoidal bleeding.
Treatment-hemorrhoidal artery embolization, termed the hemorrhoid technique. This technique involves endovascular coil occlusion of the distal branches of the SRA arising from the inferior mesenteric artery. This technique has several advantages: it leaves the hemorrhoidal tissue in place, preserves anal continence, and does not involve the creation of rectal wounds (no local care required).
Obesity is a significant health issue with an overall rise in mortality; it has multiple risk factors, including hormonal effects, which play a significant role in the balance of food intake and weight gain. Ghrelin is an anabolic hormone secreted from stomach fundus and plays a significant role in this regulation. Management of obesity involves multiple interventions, including lifestyle adjustment, pharmacotherapy, and bariatric surgery. Bariatric embolization is a relatively new procedure; several studies show that embolization of the left gastric artery reduces serum ghrelin and induces weight loss.
Left gastric artery embolization reduces the supply of blood to the gastric fundus and decreases serum levels of ghrelin. Early evidence suggests that this alteration in gut hormone balance leads to changes in energy homeostasis and weight reduction.
A radiologically inserted gastrostomy is a technique whereby a narrow plastic tube is placed through the skin, directly into stomach. Once in place the tube can be used to give you liquid feed directly into your stomach, to provide nutrition.
Gastrostomy provides an alternative access for nutritional support in patients with long-term impairment of oral intake. It is well tolerated for nutritional supplementation, generally provides improved quality of life.
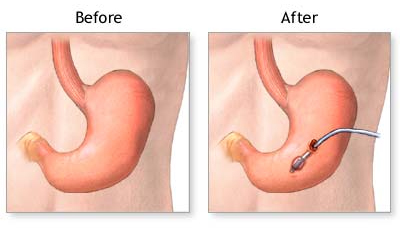
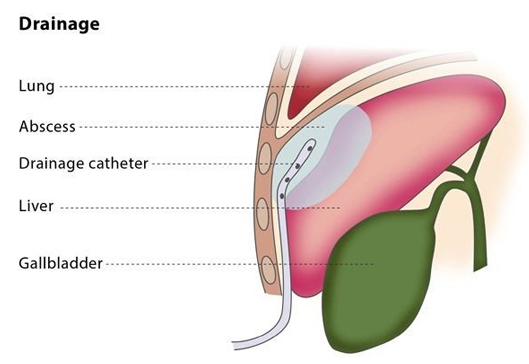
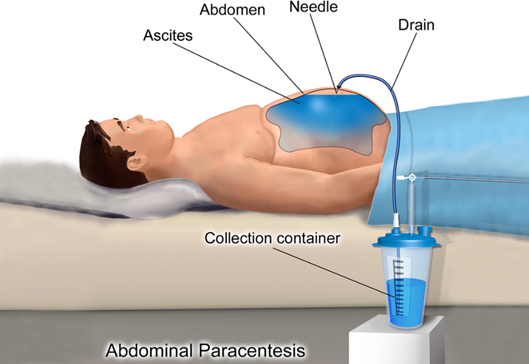
Image-guided percutaneous drainage involves using a catheter (a thin tube) to drain an abscess or a collection of fluid or air under image guidance. The interventional radiologist will insert a flexible catheter through a small cut in your skin and will guide the catheter to the collection of fluid or air. The fluid or air will then be collected in a drainage bag.
Drainage catheters are available in a variety of sizes, shapes and types. The interventional radiologist will choose the catheter according to the type of fluid, along with other factors.
If you are on any medication that prevents blood clotting, you will stop taking it before the procedure, if possible.
You should not eat anything for at least four hours before the procedure starts. You may be asked to fast for longer, depending on the puncture and difficulty of your particular case. Before the procedure, the interventional radiologist will usually place a needle in your vein to make access easier during the procedure.
Percutaneous drainage is recommended to treat fluid or air collections which produce symptoms (such as pneumothorax, which is the collection of air or gas in the gap between the chest wall and the lungs). It can also treat recurrent fluid collections by using medication and is a minimally invasive method of draining abscesses.
This procedure may not be suitable for you if you suffer from a blood clotting disorder or if the interventional radiologist cannot find a safe access route for the catheter.
The percutaneous drainage procedure cures infected fluid/air collections in over 80% of patients, though failure occurs in 5-10% of patients.
Because of the wide range of types of uninfected collections, the success rate of drainage for uninfected collections is highly variable.
A small flexible tube goes down your nose to the back of your throat, down your food pipe (oesophagus) and into your stomach.
The majority of nasogastric tubes are inserted on the ward level OR the tubes may be placed in theatre at the time of surgery.
The majority of nasogastric tubes are inserted on the ward level OR the tubes may be placed in theatre at the time of surgery.
Together with the use of water-soluble contrast media and over-the-wire technique, fluoroscopy-guided placement of nasogastric feeding tubes offers a higher rate of technical success while decreasing procedure time as well as the incidence of procedure-related complications.
The majority of nasogastric tubes are inserted on the ward level OR the tubes may be placed in theatre at the time of surgery.
In difficult cases, tube insertion is undertaken under fluoroscopic guidance.
Together with the use of water-soluble contrast media and over-the-wire technique, fluoroscopy-guided placement of nasogastric feeding tubes offers a higher rate of technical success while decreasing procedure time as well as the incidence of procedure-related complications.
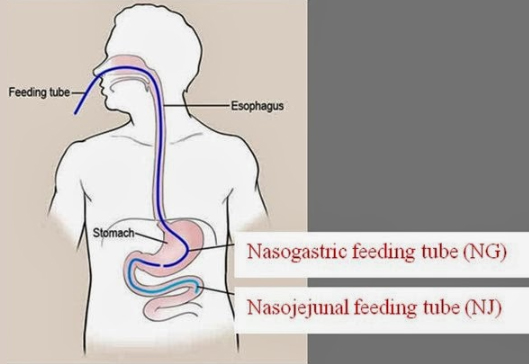
You may need a feeding tube if you cannot eat or drink enough through your mouth to meet your nutrition needs. These tubes are generally used for a short time.
A small flexible tube goes down your nose, to the back of your throat, down your food pipe (oesophagus), through your stomach and into your small intestine (jejunum). A NJ tube is used when you can’t use your stomach.
In difficult cases, tube insertion is undertaken under fluoroscopic guidance.
Together with the use of water-soluble contrast media and over-the-wire technique, fluoroscopy-guided placement of nasojejunal feeding tubes offers a higher rate of technical success while decreasing procedure time as well as the incidence of procedure-related complications.
Biopsy and Fine Needle Aspiration Cytology (FNAC) are both diagnostic procedures used to obtain tissue or cellular samples for laboratory analysis. Biopsy involves the removal of a small piece of tissue, whereas FNAC involves inserting a thin needle into the area of interest to obtain a sample of cells. Both procedures are used to diagnose cancer, infections, and other conditions. The choice of procedure depends on the location and size of the abnormality, as well as the clinical situation. Biopsy is generally more invasive and may require sedation or local anesthesia, while FNAC is less invasive and usually does not require anesthesia.
Both biopsy and FNAC procedures involve obtaining a sample of tissue or cells from the body for laboratory analysis.
In a biopsy procedure, a small piece of tissue is removed from the body using a special needle or a surgical instrument. The tissue sample is then sent to a laboratory for analysis by a pathologist, who examines it under a microscope to look for abnormal cells or tissue structures. Biopsies can be done using various methods depending on the location of the tissue to be sampled.
In an FNAC procedure, a thin, hollow needle is inserted into the area of interest, such as a lump or tumor, and a sample of cells is aspirated into the needle using a suction device. The collected cells are then smeared on a glass slide, fixed with a preservative, and sent to a laboratory for analysis. FNAC is usually performed under local anesthesia, and the procedure is generally quick and relatively painless.
Both procedures are generally safe, but they can carry some risks, such as bleeding, infection, and pain. Your doctor will explain the risks and benefits of each procedure, and help you decide which one is best for your specific situation.
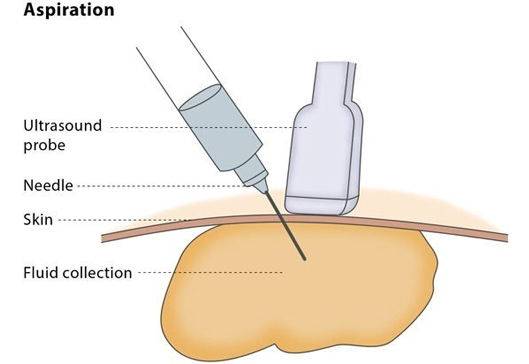
Aspiration is the image-guided puncture of a cystic lesion (such as a cyst, an abscess or bruising) or solid lesion (a growth) in order to remove a fluid or tissue sample with a suction needle. The hollow aspiration needles come in different sizes and lengths.
If you are on any medication that prevents blood clotting, you should stop taking it before the procedure, if possible.
You should not eat anything for at least four hours before the procedure. You may be asked to fast for longer, depending on the puncture and whether the procedure is particularly complicated.
The interventional radiologist may use one of a number of image guidance techniques to plan and monitor the placement of the needle during the aspiration procedure, including ultrasound, CT, MRI and fluoroscopy. You will lie down for the procedure – the exact position you will be asked to lie in depends on the access route that the interventional radiologist will use to safely approach the lesion.
Aspiration is usually performed under local anaesthesia. You may be asked to take antibiotics beforehand to reduce the risk of infection, but this is uncommon.
The procedure will be carried out in a sterile and safe environment. The interventional radiologist will use image guidance to insert a needle until the needle tip is inside the lesion. The interventional radiologist will then insert a syringe to remove the sample or cyst.
Aspiration can be performed as an in-patient or out-patient procedure. The puncture site will be monitored for 2-4 hours to check for bleeding. You may experience some mild discomfort at the puncture site during the first few hours following the procedure.
You may be recommended to have an aspiration procedure for diagnostic reasons (to provide information on the nature of the lesion) or for therapeutic purposes, such as removal of the fluid collection or cyst. Aspiration is sometimes preferred over drainage of small abscesses (less than 3-4 cm) for which a drainage catheter would be unsuitable.
Aspiration may not be the best option for you if you have a blood clotting disorder or there is no safe access route.
The technical success rate of this procedure is very high, though the clinical success rate can vary depending on the location and nature of the lesion, as well as whether the aspiration procedure is diagnostic or therapeutic.