
Nephrology and urology focus on the diagnosis and treatment of conditions affecting the kidneys, urinary tract, and male reproductive system. These systems play a crucial role in filtering waste, maintaining fluid balance, and ensuring overall body health. Any disruption can lead to complications such as infections, blockages, or impaired kidney function.
Dr. Ravi Manek offers advanced, minimally invasive, image-guided procedures to manage a wide range of urological and kidney-related conditions. These treatments help address issues like kidney stones, urinary obstructions, tumors, and fluid buildup with high precision, reduced discomfort, and lower risk compared to traditional surgery.
With a patient-centric approach, each treatment is carefully planned to restore normal function, relieve symptoms, and improve quality of life. The focus is on safe, effective care with faster recovery, minimal hospital stay, and long-term health benefits.
What is vena cava stenting?
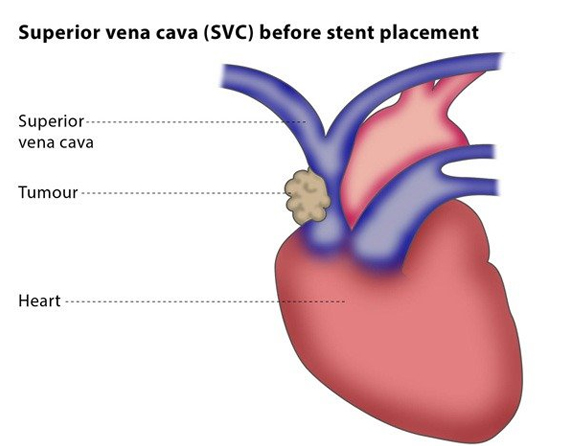
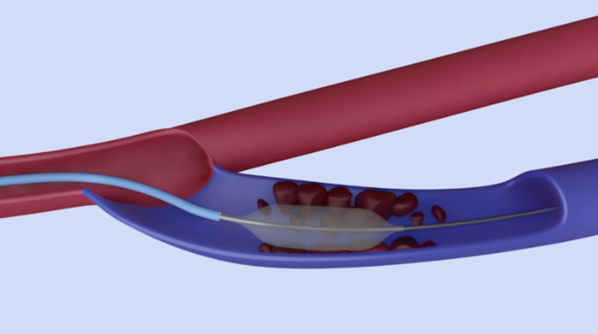
A stent is a metal mesh tube. Vena cava stents are designed for use in the superior vena cava (SVC), which transports deoxygenated blood from the upper part of the body back to the heart. In rarer cases, they are used in the Inferior Vena Cava (IVC), which carries the deoxygenated blood from the lower part of the body back to the heart.
Vena cava stenting is used to manage stenosis (narrowing) or blockage in the vein, which is most commonly caused by a malignant (cancerous) tumor. The procedure may be recommended if you are in an emergency situation, but this depends on your clinical symptoms.
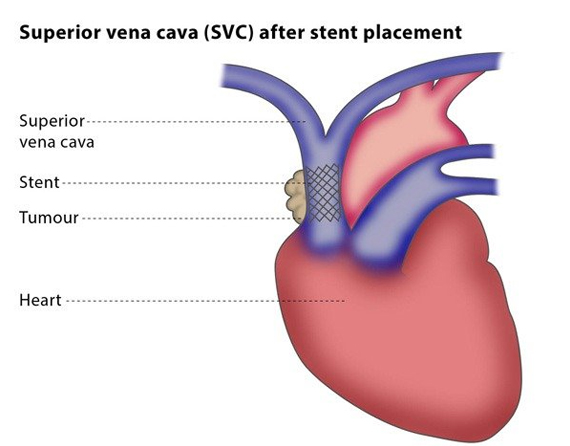
The interventional radiologist will insert a 3 mm plastic tube (called a sheath) into the base of your skull or your groin. They will then guide the sheath near the stenosis or blockage in the affected vein. The vein will be reopened using a metallic wire and a selective catheter using a technique called recanalization, after which the vena cava stent is placed.
The stent is self-expanding and acts like a skeleton to keep the vena cava open. If your vena cava is completely blocked due to a tumor, your interventional radiologist may also insert a tiny balloon that inflates once it is in the vein before and after inserting the stent. You will need to take medication that prevents blood clotting for 1-2 weeks following the procedure; the exact time period depends on the type of stent used and your clinical situation.
The aim of vena cava stenting is to manage symptoms caused by an obstruction of the blood flow in the vein, which is much more common in the SVC than in the IVC.
The main symptom of an obstructed blood flow in the vena cava is shortness of breath, followed by swelling of the face, neck, or arms, a headache, cough, and enlargement of the veins in the neck, chest, and arms. You may experience other symptoms but they are rare.
Your symptoms should stop within 48 hours of the stent placement.
There are some minor risks, including the risk of infection and bruising at the puncture site in your neck or groin. Major risks include the risk of the stent accidentally going into the heart during placement, the development of a blood clot, or the stent later becoming blocked due to a tumor, though in this case the vessel can be reopened in a second intervention.
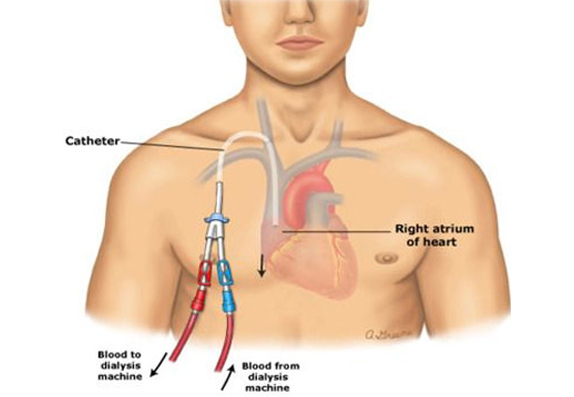
A permacath is a piece of plastic tubing – very similar to a jugular catheter – and is used in the same way for your hemodialysis.
The permacath has a cuff that holds the catheter in place and acts as a barrier to infection. The cuff is underneath the skin and cannot be seen. The catheter part that you can see is the part that protrudes from the chest wall. It is about 6 inches/15 cm long and is made of soft, white, flexible plastic. There are 2 limbs.
A transparent dressing will be put over the part where the catheter leaves the chest wall and(since the catheter is under the level of your collar bone) it will not be seen when you are clothed.
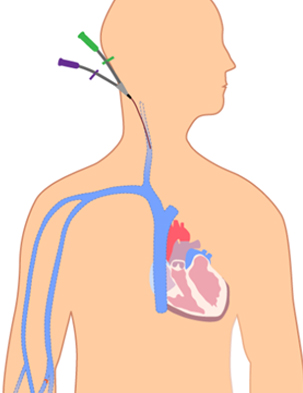
If you need hemodialysis right away and you do not have time to wait for a fistula or graft to work, the interventional radiologist can put in a catheter. The catheter is put into a vein in the neck, chest, or upper leg. This catheter is temporary. It can be used for dialysis while you wait for a fistula or graft to heal.
AV fistula is created in the forearm or arm for hemodialysis in Chronic kidney disease patients. A superficial vein of the upper limb is connected to the artery so that once the fistula mature vein can be punctured for dialysis.
The patient may present with the poor flow during dialysis due to stenosis/occlusion of a vein (common) or artery forming the fistula. A patient may also present with upper limb and or face swelling, chest pain, or heaviness due to occlusion of a major central vein.
Endovascular treatment includes angioplasty where narrowed / occluded segment is opened with a balloon. Central vein occlusion may require stenting for persistent narrowing or early recoil.
Central vein stenosis (CVS) leads to AVF outflow obstruction and venous hypertension in the affected limb which compromises the AVF patency and can result in an incapacitating upper limb edema. It is defined as a narrowing of 50% or more in the superior vena cava, brachiocephalic, or subclavian veins.
Owing to the high frequency of prior placement of an ipsilateral upper limb central venous dialysis catheter resulting in central vein injury and subsequent restorative process and stenosis, patients with end-stage renal failure (ESRF) are particularly at risk. The incidence of CVS in symptomatic ESRF patients is 16%–19% overall and 27% in those with a history of ipsilateral central venous catheter placement.
The treatment of CVS includes balloon angioplasty/stenting of the stenosed/occluded vein.
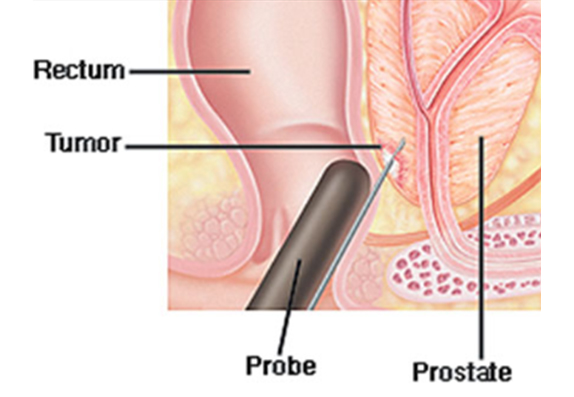
The prostate is beneath the bladder and in front of the rectum. It’s a walnut-shaped gland that surrounds part of the urethra. (That’s the tube that carries pee and semen out of the penis). Here’s what it does:
If it gets too big, your prostate can block pee from passing through the urethra and out the penis
Your doctor may order a biopsy if your prostate-specific antigen (PSA) level in your blood work is elevated or if there is an abnormal lump found during a digital rectal exam. During a digital rectal exam, your doctor inserts a finger up your bottom to feel if your prostate is enlarged or has bumps. Another option before a biopsy is an ultrasound. Instead of a finger, a small probe is inserted to take pictures of the prostate.
Once it is decided to do a prostate biopsy, it’s a simple, 10-minute procedure. An interventional radiologist inserts a needle through the wall of your rectum and into the prostate to extract the cells for testing. This is a “transrectal biopsy.” Doctors usually take a dozen samples from various parts of the prostate to rule out cancer.
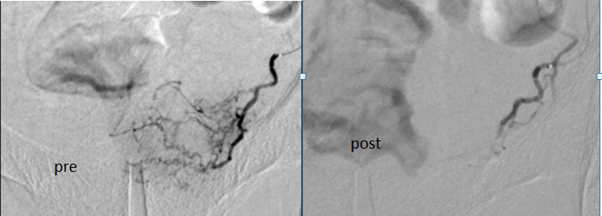
Many of the renal tumors that have a large and extensive blood supply.
Sometimes excision surgery is more difficult and risky due to high vascularity, large size, and invasion of adjacent blood vessels or organs.
24-48 hrs before surgery angioembolisation is planned, by which the blood supply of the tumor is completely stopped or decreased.
In angioembolisation, a catheter is placed into an artery (usually in the leg) and reaches arteries supplying the tumor. Material is injected to block off the blood supply to the tumor. There are many different kinds of materials available for this, depending on the type of tumor, its location, and the size of the blood vessels.
Preoperative renal artery embolization can minimize the blood loss associated with nephrectomy and also minimizes post-infarction syndrome which ultimately reduces hospital costs compared with traditional nephrectomy / laparoscopic nephrectomy approaches.
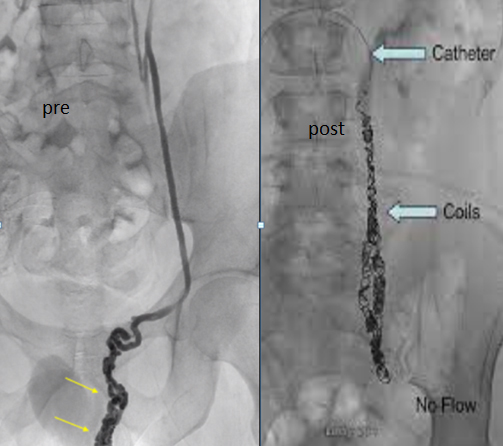
A varicocele is an enlargement of the veins in your scrotum. To ensure that blood flows in only one direction, these veins have valves that prevent blood from flowing backward. If you have a varicocele, this means that these valves are not working, causing blood to remain stagnant in the scrotum. It is similar to a varicose vein, which can occur in the legs.
If you have a varicocele, this may affect your fertility, as varicoceles can cause low sperm production, decreased sperm quality, and testicular atrophy.
Generally, varicoceles are asymptomatic, meaning that patients do not experience any symptoms, but in some cases, they can cause pain, which can vary from dull, heavy discomfort to sharp pain.
If you do experience pain, you may find that the pain increases with exercise and movement and that it gets worse over time, as symptoms often get worse over the course of the day. You may experience relief from the pain when you lie on your back.
Your doctor can diagnose you using Ultrasound or after a physical examination. The varicocele will look like a mass in the scrotum.
If you have a clinical examination, you will be asked to take a deep breath and hold it while your doctor feels the scrotum above your testicle. Alternatively, your doctor may use ultrasound to examine the dilation of the veins or to measure the blood flow. These methods allow your doctor to diagnose your varicocele.
If you experience pain, infertility, or testicular atrophy caused by a varicocele, you may undergo treatment for it. There are two main options for the treatment of a varicocele.
Surgical repair of a varicocele involves a surgeon cutting the veins which supply blood to the varicocele, meaning no blood can reach it. It may be performed under local or general anesthetic.
Minimally invasive percutaneous Embolization is a procedure in which an interventional radiologist will insert a special catheter (tube) into your groin or arm and guide this under imaging to the affected vein. The interventional radiologist will then use a liquid agent or tiny metal coils to block blood flow to the vein with the varicocele. This treatment is as effective as surgery but has less risk, pain, and recovery time.
Renal artery stenting is a procedure in which a stent is placed in the renal artery. This is helpful to treat renal artery disease.
Renal artery disease is caused by the narrowing of the arteries leading to one or both kidneys. This narrowing can also be called stenosis. It is usually caused by a build-up of fat or calcium deposits called plaque. Over time this plaque can lead to total blockage of an artery.
Due to blockage of the renal artery, the kidney doesn’t receive sufficient blood supply which activates renin – the angiotensin system, and ultimately leads to increase blood pressure, which not maintain by two or three antihypertensive medicines.
A minimally invasive procedure performed by an Interventional radiologist through the groin. A thin tube was inserted (Catheter) into the artery and a small balloon inflated in the artery. The balloon has a small mesh tube called a stent wrapped around it. It expands the stent in the artery which keeps the artery open and helps prevent further narrowing.
Renal artery stenting can be improved blood flow toward the kidney and gradually decrease blood pressure and the requirement of excessive medications.
Radiofrequency ablation (RFA) and microwave ablation (MWA) are treatments that use image guidance to place a needle through the skin into a renal tumor.
In RFA, high-frequency electrical currents are passed through an electrode, creating a small region of heat.
In MWA, microwaves are created from the needle to create a small region of heat.
The heat destroys the lung cancer cells.
RFA and MWA may be used to treat renal tumors or provide palliative care.
They are effective treatment options for patients who might have difficulty with surgery and for those for whom surgery is not an option due to metastasis.
The procedure is typically performed on an outpatient basis or with overnight observation in the hospital with general anesthesia.
Ablation can be used to treat multiple tumors simultaneously. The procedure can be repeated if new cancer appears.
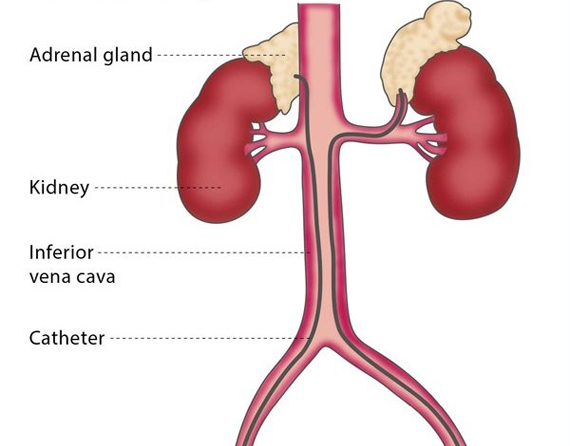
You may be recommended to undergo selective venous sampling if your doctor would like to find out more about your hormones. The procedure involves taking a sample of blood from a particular area of blood vessels, which is then analyzed to see which substances the organs and tissues around it have produced.
The organs most frequently analyzed in this procedure are the adrenal glands, the parathyroid glands, and pancreas.
The interventional radiologist will insert a 2-3 mm catheter (tube) into a blood vessel in your groin and will then use imaging to guide the catheter to the selected area of veins. The interventional radiologist then takes some samples of blood from these veins, which are immediately analyzed to check the levels of particular hormones and other substances.
Selective venous sampling is performed when it is suspected that a patient has a tumor but the doctors have been unable to find it using imaging, usually because the tumor is too small. The procedure allows surgeons to know precisely where the tumor is due to the level of hormones and other substances in the blood.