Hepato-biliary care focuses on conditions affecting the liver, gallbladder, and bile ducts—organs essential for digestion and detoxification. Disorders such as bile duct blockages, liver tumors, infections, and jaundice require timely and precise intervention to prevent complications.
Dr. Ravi Manek offers advanced, minimally invasive, image-guided procedures to diagnose and treat hepato-biliary conditions with high accuracy. Techniques such as biliary drainage, stenting, and embolization help restore bile flow, relieve symptoms, and support liver function without the need for major surgery.
These procedures ensure reduced pain, lower risk, and faster recovery, allowing patients to return to normal life sooner. Each treatment plan is carefully tailored to provide safe, effective, and long-term relief.
1. Hepatocellular carcinoma
2. To treat Selected hepatic metastasis
3. To decrease the size of tumor as a bridge to liver transplantation.
The procedure can’t be done if there are extensive metastatic disease in the liver, encephalopathy or large amount of extra hepatic metastasis. Also the procedure need special precautions in patients with liver failure, portal vein thrombosis and bleeding disorders.
1. Bleeding
2. Infection
We will keep you under overnight observation to look for any complications. After discharge, you will be called for follow-up for CT/MRI imaging to see the response of tumor to the procedure.

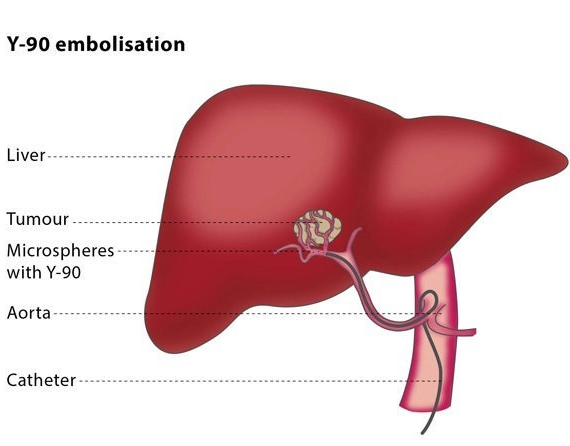
Y-90 radioembolisation is a palliative treatment for primary liver lesions and liver metastatic disease which uses ionising radiation to shrink tumours. It is generally used to relieve the symptoms of liver tumours rather than to cure the underlying condition.
The liver has two sources of blood supply: the hepatic artery and the portal vein. Liver tumours tend to rely on the hepatic artery for their blood supply.
During a radioembolisation procedure, an interventional radiologist injects microspheres filled with the radioactive isotope yttrium (known as Y-90) into the vessels feeding the tumour. Because the radiation is focused only on the tumour, higher and more effective radiation doses can be used compared to other treatments.
Depending on your individual situation, you may be given the procedure as an out-patient or you may require hospital admission following the treatment. The interventional radiologist will carry out the procedure using fluoroscopic guidance.
You will be given a local anaesthetic. After this, the interventional radiologist will insert a catheter (a thin tube) and a guidewire into an artery. You will then have some images taken of your upper abdominal arteries to show the exact location of the vessels feeding the tumour. The interventional radiologist will then insert microspheres filled with Y-90 into these vessels to deliver a high dose of radiation to the cancer cells. This radiation dose will decrease over the following two weeks.
Your vital functions will be monitored during the procedure. You may be given antibiotics to prevent infection, and, if necessary, IV analgesics or medication to prevent nausea.
If you have an inoperable liver tumour or if you are not fit for surgery, you may benefit from Y-90 radioembolisation. Y-90 is beneficial for hepatocellular carcinoma (the most common type of cancer) affecting the portal vein of the liver, or if you have not responded to chemoembolisation.
Because the radiation dose is delivered directly to the tumour, the dose is higher than in standard radiation therapy and there are fewer possible complications. Radioembolisation can extend the patient’s life expectancy from months to years, as well as improving quality of life. In some patients, this procedure enables them to undergo surgery or liver transplantation.
Y-90 radioembolisation is a relatively safe procedure. The most common complication is post-radioembolisation syndrome, which occurs in around 50% of patients. Symptoms include fatigue, low-grade fever, nausea, vomiting and abdominal discomfort.
Less common complications include a build-up of fluid, high levels of alkaline phosphatase and infection. You may also experience stomach ulcers, inflammation of the pancreas, raised blood pressure, gallbladder inflammation or pneumonia. As with all percutaneous procedures, there is a risk of bleeding or damage to a blood vessel.
In some cases, patients react to the iodinated contrast materials used in the procedure, experiencing allergic reactions and harmful effects on the kidneys
Percutaneous Ethanol Injection (PEI) was an early technique involving the injection of absolute ethanol (alcohol) directly into HCC lesions under ultrasound control and achieved satisfactory results in small tumours less-then 3cm. Other techniques that have been used include cryoablation (freezing of tumours), microwave ablation, and laser techniques, but radiofrequency ablation (RFA) remains the predominant technique. RFA has been approved by NICE (National Institute of Clinical Excellence) for the treatment of unresectable HCC and colorectal hepatic metastases.
RFA produces movement of ions in the tissue which results in heating and cellular death. Heating to a temperature of 60-100°C results in almost immediate tissue damage.
RFA is based on producing tissue necrosis using a high-frequency alternating current that is delivered through an electrode placed in the centre of the tumour. Tissue necrosis begins as the temperature approaches 60°C, and RFA treatments often result in local tissue temperatures that approach or exceed 100°C, which result in tumour cell death.
It is possible to treat single tumours of up to 5 cm in diameter, and multiple tumours of less-then 3cm diameter.
RFA may be performed either under sedation or general anaesthesia. The liver lesions will have been identified using either ultrasound (US) or computed tomography (CT), and the RFA procedure can be performed under either US or CT guidance, which is usually determined by the interventional radiologist prior to the procedure.
The procedure would normally be performed in the CT scanner or the interventional radiology suite. Once positioned upon the scanning table, the skin over the liver will be cleaned and sterilised and a sterile drape applied. Local anaesthetic is infiltrated into the overlying tissues and either sedation or general anaesthesia is required for pain relief during the procedure.
An insulated needle with an electrode at the tip is used which transmits high-frequency alternating current to the tumour tissue. The needle electrode is inserted into the tumour usually under ultrasound guidance with CT to confirm the final position.
Following ablation of the tumour, continued heating of the needle on withdrawal or “track ablation” avoids spreading of tumour cells.
Complications of RFA include haemorrhage, liver abscess, and heat injury to adjacent structures e.g. bowel and gallbladder. The use of “hydrodissection” (the injection of dextrose solution to push away other nearby organs) can be used to avoid local complications or injury to other structures.
Results of RFA in HCC, either alone or in combination with TACE have been encouraging.
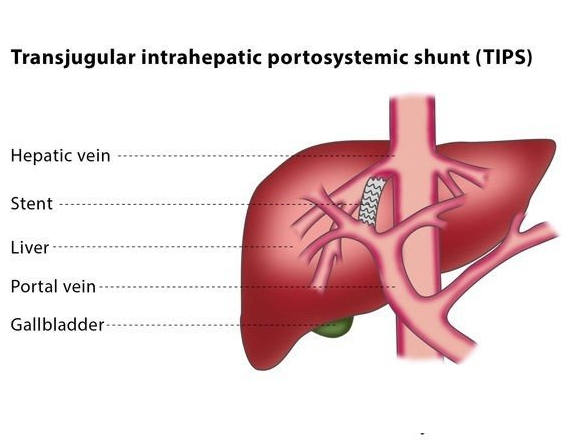
A shunt is an artificial passage which allows fluid to move from one part of your body to another. A transjugular intrahepatic portosystemic shunt (TIPS) connects the vein which brings blood from your gastrointestinal tract and intra-abdominal organs to your liver, and the vein from your liver to the right part of your heart.
You will be conscious but sedated for the procedure, which the interventional radiologist will carry out using fluoroscopy and ultrasound for guidance.
The interventional radiologist will puncture your jugular vein on the right side of your neck with a needle and will then insert a vascular sheath over a wire into the inferior vena cava. They will explore the hepatic vein with a catheter designed for this purpose.
The interventional radiologist will puncture the portal vein through the liver with a special needle and position a wire between the two veins. After the area has been dilated, a stent or stent graft will be placed between the portal and hepatic vein to create a lasting connection.
The TIPS procedure is usually performed in patients with liver cirrhosis. If you have this condition, your normal blood flow through the liver is blocked by scar tissue within the liver, which increases the pressure in your portal vein.
The increased pressure in your portal vein makes thin veins in your gullet or stomach become abnormally enlarged and so at risk of bleeding. Another symptom of liver cirrhosis is an abnormal collection of fluid (ascites) in the abdominal cavity.
The increased pressure in your portal vein makes thin veins in your gullet or stomach become abnormally enlarged and so at risk of bleeding. Another symptom of liver cirrhosis is an abnormal collection of fluid (ascites) in the abdominal cavity.
Once the interventional radiologist has placed the shunt, the pressure in the portal vein decreases, protecting the area from bleeding and reducing the ascites.
Because a liver suffering from cirrhosis is shrunken and the liver tissue can be very hard, it is possible to puncture the outside of the liver. This can cause bleeding which requires further treatment.
Another risk is that after the TIPS procedure ammonia from the intestine might bypass the liver and be delivered to the brain, which may result in a condition called hepatic encephalopathy, the symptoms of which range from mild (alterations in thinking) to severe (confusion and coma).
Due to the shunt, there is an increased amount of blood flowing directly to the heart, which can cause heart failure. If you experience this, your doctor will decrease or disrupt the blood flow through the TIPS.
You will be conscious but sedated for the procedure, which the interventional radiologist will carry out using fluoroscopy and ultrasound for guidance.
The interventional radiologist will puncture your jugular vein on the right side of your neck with a needle and will then insert a vascular sheath over a wire into the inferior vena cava,with a catheter designed for this purpose.
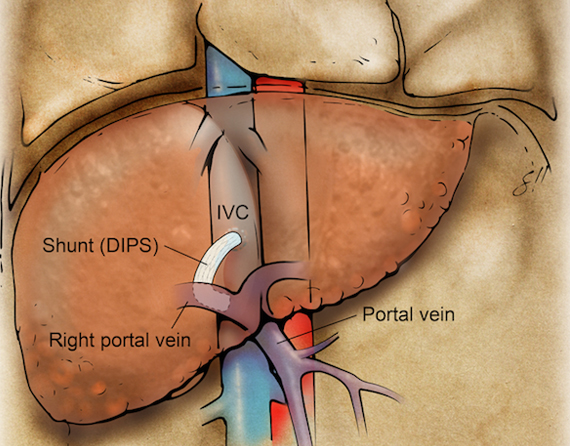
The interventional radiologist will puncture the Inferior venacava(IVC) through the liver with a special needle and position a wire between the two veins. After the area has been dilated, a stent or stent graft will be placed between the portal and IVC to create a lasting connection.
The DIPS procedure is usually performed in patients with liver cirrhosis. If you have this condition, your normal blood flow through the liver is blocked by scar tissue within the liver, which increases the pressure in your portal vein.
The increased pressure in your portal vein makes thin veins in your gullet or stomach become abnormally enlarged and so at risk of bleeding. Another symptom of liver cirrhosis is an abnormal collection of fluid (ascites) in the abdominal cavity.
You may be advised to undergo DIPS if you have varices which bleed acutely or recurrently and have not responded to other treatments.
Once the interventional radiologist has placed the shunt, the pressure in the portal vein decreases, protecting the area from bleeding and reducing the ascites.
Because a liver suffering from cirrhosis is shrunken and the liver tissue can be very hard, it is possible to puncture the outside of the liver. This can cause bleeding which requires further treatment.
Another risk is that after the DIPS procedure ammonia from the intestine might bypass the liver and be delivered to the brain, which may result in a condition called hepatic encephalopathy, the symptoms of which range from mild (alterations in thinking) to severe (confusion and coma).
Another risk is that after the DIPS procedure ammonia from the intestine might bypass the liver and be delivered to the brain, which may result in a condition called hepatic encephalopathy, the symptoms of which range from mild (alterations in thinking) to severe (confusion and coma).
Diagnosis of liver disease
Characterization of liver disease often requires a liver biopsy. Liver biopsy can be performed by standard approach (by passing a needle directly through the body wall and into the liver) or by transjugular approach. The transjugular approach is favored in patients who have high bleeding risk because it does not require passing a needle through the liver capsule (the surface of the liver).
An interventional radiologist uses ultrasound and X-rays to puncture the jugular vein and advance a small sheath into the vein draining the liver (hepatic vein). Through the sheath, a biopsy needle is passed through the vein wall and into the surrounding liver tissue to obtain samples. By using this technique, any bleeding that occurs from the biopsy will bleed into the hepatic vein, meaning no loss of blood by the patient.
Conscious sedation
There is still some risk of bleeding, if the biopsy needle passes into an artery or beyond the liver capsule. Small risk of infection or damage to surrounding structures.
Two hours of bed rest.
The results of the biopsy will be available to your referring physician in 1-3 days.
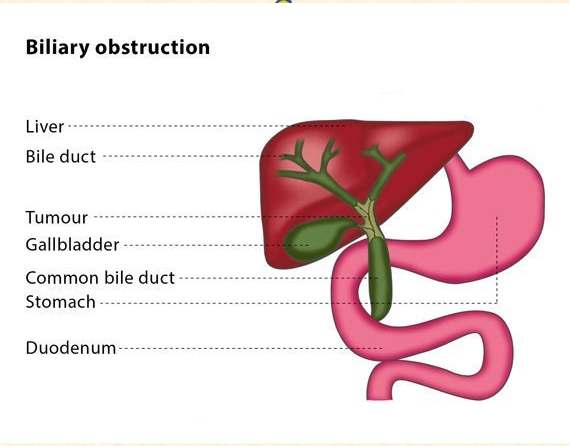
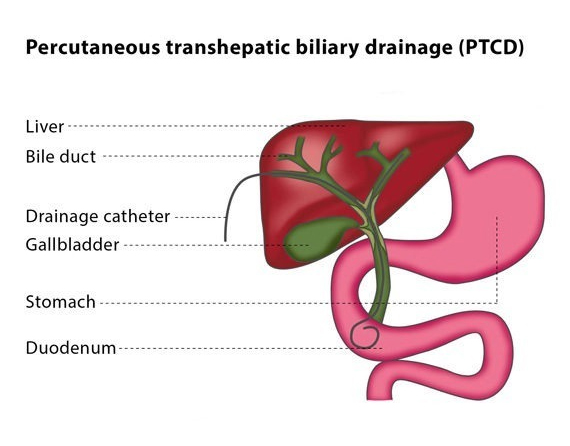
Percutaneous transhepatic biliary drainage (PTCD) is the placement of a drain into bile ducts using needles inserted through the skin. The procedure can be used to treat cholestasis (where the bile cannot flow from the liver to the small intestine), which may be a result of a narrowing or blockage in the bile ducts or of a bile leakage after an operation.
Puncturing the bile duct is usually performed under sedation and local anaesthesia, though in rare cases and depending on the patient’s underlying condition and age, the procedure may be carried out under general anaesthesia.
You will be given antibiotics beforehand to prevent infection. The procedure will be carried out in a sterile room while you lie on your back. The interventional radiologist will perform the procedure under X-ray guidance, though sometimes ultrasound is used in addition to fluoroscopy to confirm the direction for the puncture.
The interventional radiologist will pass a small needle through your skin into either your left or your right liver lobe. If it is the right liver lobe which is punctured, this will be between your ribs and in the middle of your side. If it is your left liver lobe which is punctured, the interventional radiologist will choose an entry site below the tip of your breastbone.
As the needle is withdrawn, the interventional radiologist will gently inject a diluted contrast agent, a substance which makes the area show up better under imaging. This means that, when the needle enters the bile duct, the tubular structure is more clearly visible under imaging. The interventional radiologist will then insert a guidewire into the bile duct, which is followed by a catheter. The guidewire and catheter are used together to move past the blockage and reach the intestine.
Once the interventional radiologist has removed this catheter, they will dilate the blocked liver tract so that the drainage catheter can be placed. A drainage catheter has multiple holes in its side which are used to drain the bile in two directions, outwards into a bag and inwards into the intestine. The bag will be attached to the skin and left in place for a few days until the biliary tract has decompressed. During the period when the bag is attached, the catheter is flushed 2-3 times a day with sodium chloride to keep the side-holes open.
If you are unsuitable for endoscopic procedures, PTCD is a possible alternative for you. It can be used to decompress the biliary ducts if they are blocked by a mass lesion or a stone, or to bridge a hole if you experience bile leakage.
One of the most common complications is bleeding into the biliary tract, usually from a vein. This normally does not need treatment as it heals by itself. A less frequent complication is major bleeding requiring a blood infusion or further interventions, such as surgery or embolisation of the vessels.
If you have a biliary infection, the PTCD procedure may cause fever, chills and septicaemia. A further risk is the possibility that the areas around the tract will be punctured during the procedure, such as the gallbladder or bowel.
Percutaneous transhepatic biliary drainage (PTCD) is the placement of a drain into bile ducts using needles inserted through the skin. The procedure can be used to treat cholestasis (where the bile cannot flow from the liver to the small intestine), which may be a result of a narrowing or blockage in the bile ducts or of a bile leakage after an operation.
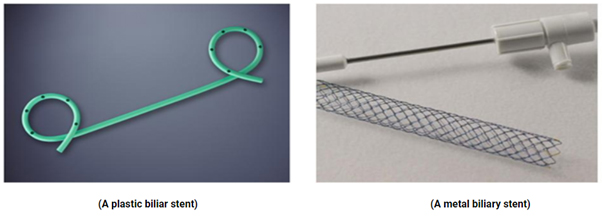
Biliary stenting is performed after biliary drainage if the blockage is malignant (cancerous) to keep the bile duct open and to allow the drain used in PTCD to be removed. This involves putting a stent (a mesh metal tube) into the bile duct, which then functions as a supportive skeleton to prevent the duct from closing.
Puncturing the bile duct is usually performed under sedation and local anaesthesia, though in rare cases and depending on the patient’s underlying condition and age, the procedure may be carried out under general anaesthesia.
You will be given antibiotics beforehand to prevent infection. The procedure will be carried out in a sterile room while you lie on your back. The interventional radiologist will perform the procedure under X-ray guidance, though sometimes ultrasound is used in addition to fluoroscopy to confirm the direction for the puncture.
The interventional radiologist will pass a small needle through your skin into either your left or your right liver lobe. If it is the right liver lobe which is punctured, this will be between your ribs and in the middle of your side. If it is your left liver lobe which is punctured, the interventional radiologist will choose an entry site below the tip of your breastbone.
As the needle is withdrawn, the interventional radiologist will gently inject a diluted contrast agent, a substance which makes the area show up better under imaging. This means that, when the needle enters the bile duct, the tubular structure is more clearly visible under imaging. The interventional radiologist will then insert a guidewire into the bile duct, which is followed by a catheter. The guidewire and catheter are used together to move past the blockage and reach the intestine.
Once the interventional radiologist has removed this catheter, they will dilate the blocked liver tract so that the drainage catheter can be placed. A drainage catheter has multiple holes in its side which are used to drain the bile in two directions, outwards into a bag and inwards into the intestine. The bag will be attached to the skin and left in place for a few days until the biliary tract has decompressed. During the period when the bag is attached, the catheter is flushed 2-3 times a day with sodium chloride to keep the side-holes open.
If you are unsuitable for endoscopic procedures, PTCD is a possible alternative for you. It can be used to decompress the biliary ducts if they are blocked by a mass lesion or a stone, or to bridge a hole if you experience bile leakage.
One of the most common complications is bleeding into the biliary tract, usually from a vein. This normally does not need treatment as it heals by itself. A less frequent complication is major bleeding requiring a blood infusion or further interventions, such as surgery or embolisation of the vessels.
If you have a biliary infection, the PTCD procedure may cause fever, chills and septicaemia. A further risk is the possibility that the areas around the tract will be punctured during the procedure, such as the gallbladder or bowel.
The liver has the ability to grow back the pieces that have been removed, as long as not too much tissue is removed at once. Approximately 30 to 40% needs to remain. If there is less than that left after liver surgery, a portal embolization can ensure that the part of the liver that will remain in the body can grow before the procedure. A portal vein embolization is a procedure intended to stimulate liver growth. This procedure will be necessary if not enough liver tissue is expected to remain after surgery. During embolization, the blood flow to the area is blocked. Portal vein embolization blocks the blood flow to certain parts of the liver using small particles, glue, small metal coils, and/or a plug. The material is administered into the vein by an interventional radiologist using a needle and catheter (small, flexible tube) using image-guided techniques.
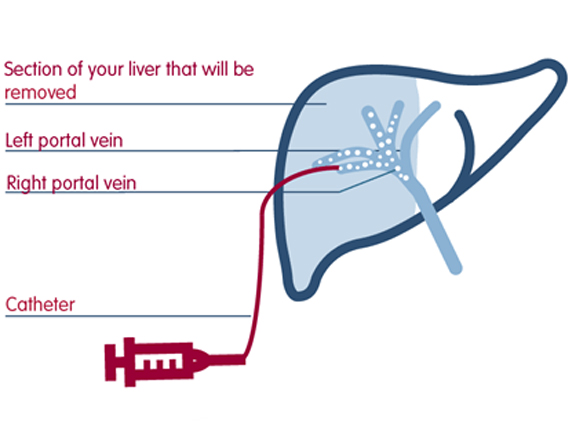
Illustration portal vein embolization
If you are eligible for a portal vein embolization, you will be referred to an interventional radiologist who can provide more information about the procedure. You will most likely be able to see their anesthesiologist that same day, to see if you are in good enough shape to handle the sedative.
Please inform your practicing physician if you use medication that prevents blood coagulation. If possible, you will have to stop using this medication before the procedure. You will probably have to spend one night at the hospital. Please do not eat solid foods 8 hours before the procedure, and only drink clear liquids. Please do not drink anything 4 hours before the procedure,
Your specialized anesthesiologist will put you to sleep before the procedure. The procedure will take place at the radiology department. You will be lying down on your back with an x-ray tube. This table is designed for use with image-guided procedures.
Guided by ultrasound and x-ray, your interventional radiologist will puncture the portal vein through your sides or epigastrium. We will make scans using a contrast agent to map out the anatomy of the portal vein. Then the interventional radiologist will close the part of the portal vein that won’t be necessary anymore using microparticles, glue, small metal coils, and/or a plug. After your treatment, the area of the puncture will be closed using glue or a small plug.
You can wake up peacefully in the recovery room after your procedure. Once you are properly awake, you can return to your ward. Most patients can go home the next day. Approximately 3 to 4 weeks after your procedure, you will come back for a new CT (and MRI) scan to assess whether the liver has sufficiently grown and whether hepatic surgery is an option for you.
Most people experience mild pain on the side of the liver after the procedure. If necessary, we can give you some painkillers to take home. A few people may experience nausea or vomiting, abdominal pain, and feel. This should pass with time.
Hematoma near the puncture spot
Hemorrhaging. This may cause pain, dizziness, or transpiration. Please notify your nurse if this happens to you.
Varices are dilated vessels which may rupture, causing variceal bleeding. Gastric variceal bleeding describes the bleeding that occurs when dilated vessels in the stomach rupture, and is associated with high morbidity and mortality rates. One of the major possible complications of portal hypertension is gastric variceal bleeding; portal hypertension refers to high blood pressure in the liver. BRTO/CARTO/PARTO are minimally invasive techniques used to treat gastric variceal bleeding.
Balloon-occluded retrograde transvenous obliteration (BRTO)
Coil-assisted retrograde transvenous obliteration (CARTO)
Plug-assisted retrograde transvenous obliteration (PARTO)
Balloon-occluded retrograde transvenous obliteration (BRTO)
Portal hypertension refers to high blood pressure in the liver. One of the major possible complications of portal hypertension is gastric variceal bleeding. Varices are dilated vessels which may rupture, causing variceal bleeding. Gastric variceal bleeding describes the bleeding that occurs when dilated vessels in the stomach rupture, and is associated with high morbidity and mortality rates.
BRTO is a minimally invasive technique that is used to treat gastric variceal bleeding. The procedure involves blocking the dilated vessels, reducing the risk of rupture. It can be used in addition to or as an alternative to TIPS, which is the primary treatment for gastric varices. TIPS aims to relieve the pressure on the dilated vessels by creating new connections between blood vessels in the liver using a shunt.
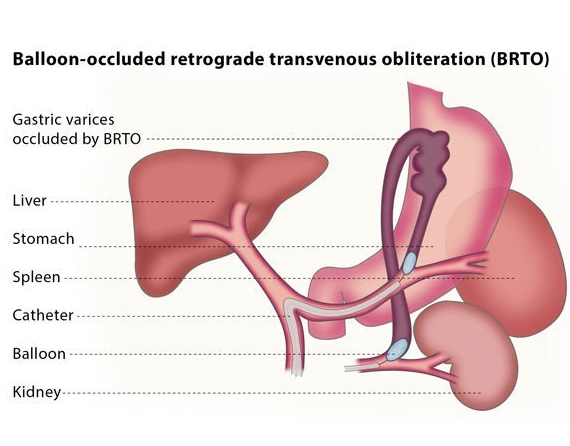
The interventional radiologist will insert a balloon catheter (a thin, flexible tube with a tiny balloon at one end) through a vein in your thigh or neck and guide the catheter to the liver using fluoroscopy for guidance. The catheter is then directed to the gastrorenal or gastrocaval shunt and the balloon is expanded to block the shunt.
The interventional radiologist will then perform a venography, which is a type of imaging technique in which X-rays are used to see the vessels clearly. This will allow the interventional radiologist to confirm exactly which vessels need to be treated and if there are any other abnormal or dilated vessels which have not previously been identified. A medication will then be injected into the dilated vessels through the catheter, until they are completely filled. This medication will remain in the vessel for a short period of time, and will then be removed under fluoroscopy.
Another venography will then be performed, to confirm that the blood flow in the shunt has stopped. Finally, the balloon will be deflated and the interventional radiologist will withdraw the catheter.
You may be advised to undergo this procedure if you are at risk of or already have gastric variceal bleeding and hepatic encephalopathy as well as a gastrorenal shunt. Hepatic encephalopathy refers to the worsening of brain function that is caused by a damaged liver.
Although TIPS has been considered the standard therapy for gastric varices that have been unresponsive to other treatments, recent reports have stated that BTRO is a less invasive and more effective way to manage varices than shunt surgery or TIPS. TIPS does not always cause the disappearance of gastric varices, while BRTO can in most cases completely destroy these vessels.
BRTO has tended to be used to prevent gastric variceal bleeding. It is also an effective therapy for sclerosis (narrowing) of new portosystemic shunts with the additional complication of hepatic encephalopathy. One of the greatest advantages of BRTO is its preservation of liver function. Moreover, the increase of blood flow in BRTO can also improve liver function in cases where the patient has cirrhosis (scarring of the liver).
Procedure-related complications are minor and include bleeding and infection. In rare cases, the blockage of the blood to the gastric varices can further increase the pressure on the liver, causing damage to the liver.
The most serious complications of the procedure, however, are related to the medication used to block the vessels, which is called ethanolamine oleate. Inflow of a relatively large amount of ethanolamine oleate can lead to serious complications. These complications include pulmonary embolism (blockage in a lung’s main artery), fluid in or around the lungs, hypersensitivity, fever, problems with blood flow to the heart and the formation of small blood clots in vessels throughout the body. Ethanolamine oleate also causes haemolysis, which is the rupturing of red blood cells.
To prevent this from occurring, only a low dose of the medication is used.
Coil-assisted retrograde transvenous obliteration (CARTO) and Plug-assisted retrograde transvenous obliteration (PARTO)
Are similar to BARTO only difference is that Coils/Plug are used instead of balloon respectively
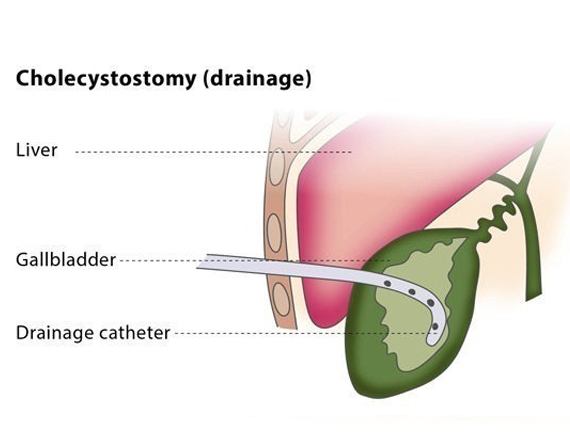
It is an image-guided placement of drainage catheter into gallbladder lumen. This minimally invasive procedure can aid the stabilization of a patient to enable a more measured surgical approach with time for therapeutic planning.
The gallbladder is punctured with an 18 or 19 gauge needle under ultrasound guidance. Bile can then be aspirated for microbiological studies. A 0.035 guidewire is used to exchange the needle for a dilator and an 8 French or larger pigtail drain is placed within the gallbladder. The drain can often be visualized under ultrasound. Aspiration of bile/pus from the drain confirms satisfactory position.
Poor surgical candidate / high-risk patients with acute calculous or acalculous cholecystitis
Unexplained sepsis in critically ill patients (diagnostic for cholecystitis as etiology of sepsis if clinical improvement after cholecystostomy)
Access to or drainage of biliary tree following failed ERCP and PTC
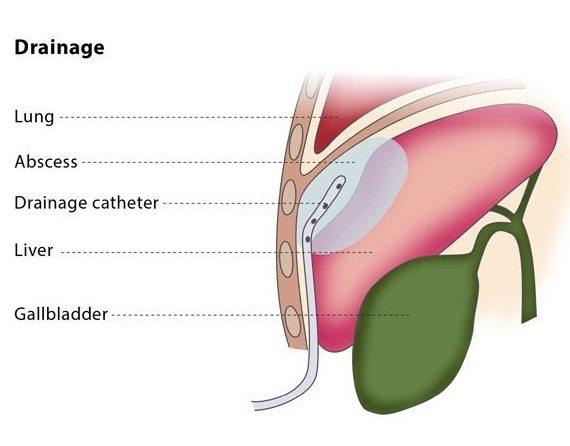
Image-guided percutaneous drainage involves using a catheter (a thin tube) to drain an abscess or a collection of fluid or air under image guidance. The interventional radiologist will insert a flexible catheter through a small cut in your skin and will guide the catheter to the collection of fluid or air. The fluid or air will then be collected in a drainage bag.
Drainage catheters are available in a variety of sizes, shapes and types. The interventional radiologist will choose the catheter according to the type of fluid, along with other factors.
If you are on any medication that prevents blood clotting, you will stop taking it before the procedure, if possible.
You should not eat anything for at least four hours before the procedure starts. You may be asked to fast for longer, depending on the puncture and difficulty of your particular case. Before the procedure, the interventional radiologist will usually place a needle in your vein to make access easier during the procedure.
Percutaneous drainage is recommended to treat fluid or air collections which produce symptoms (such as pneumothorax, which is the collection of air or gas in the gap between the chest wall and the lungs). It can also treat recurrent fluid collections by using medication and is a minimally invasive method of draining abscesses.
This procedure may not be suitable for you if you suffer from a blood clotting disorder or if the interventional radiologist cannot find a safe access route for the catheter.
The percutaneous drainage procedure cures infected fluid/air collections in over 80% of patients, though failure occurs in 5-10% of patients.
Because of the wide range of types of uninfected collections, the success rate of drainage for uninfected collections is highly variable.
There are some risks associated with the procedure. Major complications include bacteraemia (the presence of bacteria in the blood, which occurs in 2-5% of cases) and septic shock (caused by severe infection and sepsis, which occurs in 1-2% of cases). Other complications include the risk of haemorrhage and superinfection (infection of a sterile collection of fluid, following a previous infection).
A hepatic vein stenting to relieve stenosis which causing the Budd-Chiari syndrome.
Budd-Chiari syndrome (BCS) is a liver congestion due to hepatic venous outflow obstruction at any level from the small hepatic veins to the junction of the inferior vena cava (IVC) and the right atrium so liver. Patients with BCS may present with symptoms and signs of portal hypertension, including ascites, hepatomegaly, splenomegaly, and progressive liver dysfunction.
The cause of BCS is not completely understood.
The anatomy of the hepatic veins is complex and distorted during progression of BCS; thus, it is not practical to surgically reconstruct the veins.
The anatomy of the hepatic veins is complex and distorted during progression of BCS; thus, it is not practical to surgically reconstruct the veins.
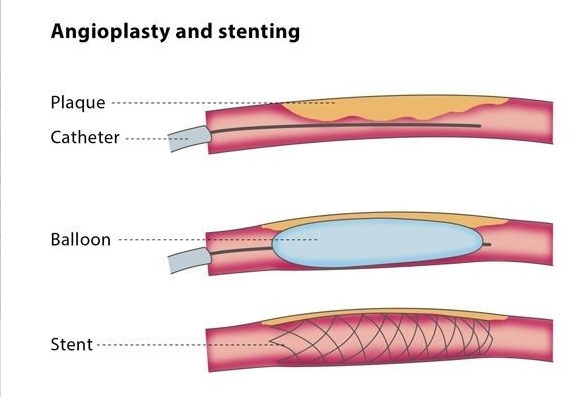
Advanced atherosclerotic obstruction or occlusion of the mesenteric artery causes Chronic Mesenteric Ischemia(CMI). Despite the high population prevalence of atherosclerosis of the mesenteric vessels, CMI may not arise until late in the disease course, due to the formation of extensive collateral vessels originating from abdominal vasculature. When primary or collateral blood supply becomes threatened as a result of obstructive disease, generally in two or more major abdominal arteries (celiac artery [CA], superior mesenteric artery [SMA], or inferior mesenteric artery [IMA]), clinical symptoms manifest and a decision towards vascular intervention in the form of stenting should be considered.
Superior mesenteric artery (SMA) embolism is a life-threatening vascular emergency that requires rapid revascularization of mesenteric blood flow as well as early diagnosis and is the most frequent cause of acute mesenteric ischemia, which is associated with a high mortality rate. treatment options include Thrombolysis, aspiration, and stent of SMA.