The lymphatic system plays a crucial role in maintaining fluid balance, supporting immunity, and removing toxins from the body. Disorders such as lymphatic blockages, leaks, or lymphedema can lead to swelling, discomfort, and increased risk of infections, requiring specialized care.
Dr. Ravi Manek offers advanced, minimally invasive, image-guided procedures to diagnose and treat lymphatic conditions with high precision. Techniques such as lymphangiography and embolization help identify and manage leaks or obstructions, improving fluid drainage and overall function.
These treatments provide effective relief with minimal discomfort and faster recovery compared to traditional approaches. Each case is carefully evaluated to deliver personalized care focused on restoring normal lymphatic flow and enhancing quality of life.
DVT is a blood clot in a vein located deep in the body. Veins in the legs are the most common place for a DVT to develop. A blood clot in leg veins is an emergency because it can lead to life-threatening complications This condition is serious because blood clots can loosen and lodge in the lungs
It occurs in patient with long time bed ridden, malignancy, on contraceptive pills, trauma, dehydration or compression of vein by artery.
Patients may present with sudden onset swelling, pain, redness or tightness of leg. Presentation with small to large pulmonary embolisation is not uncommon.
On Examinations, redness, pitting oedema & calf tenderness.
Endovascular therapy, including aspiration thrombectomy where blood clot is aspirated orcatheter directed thrombolytic therapy infusion where clot buster drug is directly infused into the thrombus with catheter.
The goal of endovascular treatment is to establish blood flow to give early symptomatic relief to patient, reduce future post thrombotic complications & reduce the chances of pulmonary embolism.
An inferior vena cava (IVC) filter is a small device that can stop blood clots from going up into the lungs. The inferior vena cava is a large vein in the middle of your body. The device is put in local anesthesia.
Veins are the blood vessels that bring oxygen-poor blood and waste products back to the heart. A deep vein thrombosis (DVT) is a blood clot that forms in a vein deep inside the body. A clot occurs when blood thickens and clumps together. In most cases, this clot forms inside one of the deep veins of the thigh or lower leg.
The veins in your legs have tiny valves that help keep blood moving back up toward the heart. But a DVT may damage one or more of these valves. This causes them to weaken or become leaky. When this happens, blood starts to pool in your legs. This can also happen if you are immobile for a long period of time. Normally, muscles in the leg help blood move up in the veins when the muscles contract. When blood flows very slowly through the veins, this increases the risk that cells in the blood will stick together and form a clot.
DVT is a serious medical condition that can cause swelling, pain, and tenderness in your leg. In some cases, a deep clot in a leg vein can break free and stick in a vessel in the lung. This can cause a blockage in the vessel called a pulmonary embolism. Pulmonary embolism can cause severe shortness of breath and even sudden death.
An IVC filter is one method to help prevent pulmonary embolism. Your inferior vena cava (IVC) is the major vein that brings oxygen-poor blood from the lower body back to the heart. The heart then pumps the blood to the lungs to pick up oxygen. An IVC filter is a small, wiry device. When the filter is placed in your IVC, the blood flows past the filter. The filter catches blood clots and stops them from moving up to the heart and lungs. This helps to prevent a pulmonary embolism.
The IVC filter is placed through a small incision in a vein in your groin or neck. A thin, flexible tube (catheter) is inserted into this vein. The catheter is then gently moved into your IVC. A collapsed IVC filter is sent with the catheter. The filter is left in place, and the catheter is removed. The filter then expands and attaches itself to the walls of the IVC. It may be removed after a period of time.
The filter helps to protect you from a life-threatening pulmonary embolism if you have a DVT.

An inferior vena cava (IVC) filter is a small device that can stop blood clots from going up into the lungs. The inferior vena cava is a large vein in the middle of your body. The device is put in local anesthesia.
Veins are the blood vessels that bring oxygen-poor blood and waste products back to the heart. A deep vein thrombosis (DVT) is a blood clot that forms in a vein deep inside the body. A clot occurs when blood thickens and clumps together. In most cases, this clot forms inside one of the deep veins of the thigh or lower leg.
The veins in your legs have tiny valves that help keep blood moving back up toward the heart. But a DVT may damage one or more of these valves. This causes them to weaken or become leaky. When this happens, blood starts to pool in your legs. This can also happen if you are immobile for a long period of time. Normally, muscles in the leg help blood move up in the veins when the muscles contract. When blood flows very slowly through the veins, this increases the risk that cells in the blood will stick together and form a clot.
DVT is a serious medical condition that can cause swelling, pain, and tenderness in your leg. In some cases, a deep clot in a leg vein can break free and stick in a vessel in the lung. This can cause a blockage in the vessel called a pulmonary embolism. Pulmonary embolism can cause severe shortness of breath and even sudden death.
An IVC filter is one method to help prevent pulmonary embolism. Your inferior vena cava (IVC) is the major vein that brings oxygen-poor blood from the lower body back to the heart. The heart then pumps the blood to the lungs to pick up oxygen. An IVC filter is a small, wiry device. When the filter is placed in your IVC, the blood flows past the filter. The filter catches blood clots and stops them from moving up to the heart and lungs. This helps to prevent a pulmonary embolism.
The IVC filter is placed through a small incision in a vein in your groin or neck. A thin, flexible tube (catheter) is inserted into this vein. The catheter is then gently moved into your IVC. A collapsed IVC filter is sent with the catheter. The filter is left in place, and the catheter is removed. The filter then expands and attaches itself to the walls of the IVC. It may be removed after a period of time.
The filter helps to protect you from a life-threatening pulmonary embolism if you have a DVT.
Lymphography is a medical imaging technique in which an interventional radiologist injects radiocontrast agent, and then an X-ray picture is taken to visualise structures of the lymphatic system, including lymph nodes, lymph ducts, lymphatic tissues, lymph capillaries and lymph vessels
During lymphangiography, the physician will place small needles into lymph nodes in the groin area. A small amount of a contrast agent (a safe, injectable dye) will be injected into the needles and tracked by, X-ray or fluoroscopy as it travels upward through the lymphatic system.
Lymphatic malformations are another type of vascular abnormality. They are often large fluid filled spaces containing lymph instead of blood. These are called macrocystic lymphatic malformations. The other type of lymphatic maiformation is “microcystic and this type contains multiple tiny spaces.
The macrocystic malformations are commonly diagnosed in childhood and can grow to be very large. They can occasionally compress nearby structures and if these are important, e.g. the trachea (windpipe), treatment may be required soon.
They are treated in a similar fashion to venous malformations using sclerotherapy and similar risks are present. The risk of this is minimal in most cases but this will be discussed with you before the procedure.
Sclerotherapy treatment involves the injection of a special chemical into the venous malformation to ultimately shrink it and relieve the symptoms it is causing. It is typically carried out as a day case procedure in hospital.
Various substances can be used but most commonly the chemical used is Sodium Tetradecyl sulphate (Fibrovein). When injected into a lesion it causes an inflammatory reaction which leads to localised blood clots and the formation of a scar in place of the venous malformation, causing the malformation to shrink.
Sclerotherapy is carried out under ultrasound and X-ray control. This allows the doctor needs to make sure that the needle goes into exactly the right place and to assess the degree of communication with veins nearby.
Often a ‘course’ of multiple injections are required to adequately treat a venous malformation and it can be some time before you notice a significant difference. Not all venous malformations are successfully treated in this way but in the vast majority of cases significant results are achieved.
Sclerotherapy is not a ‘cure’ for these malformations but is aimed at controlling symptoms and reducing the size. Sclerotherapy may not treat skin discolouration associated with some: malformations.
Venous malformations are abnormally developed blood vessels with varying degrees of communication with normal veins. They are sometimes described as abnormal ‘vascular lakes or low flow lesions. They contain venous blood, which is very slow moving.
Supporting these vascular lakes is a solid component known asa matrix. The ratio of spaces and matrix within a vascular malformation varies considerably from patient to patient. It can differ to some extent within different malformations within the same person.
Venous malformations can occur anywhere in the body and are present at birth, although they may not become apparent until later in life. Other situations when they may be come apparent are following episodes of local trauma (injury), at puberty, or during pregnancy — due to hormonal changes occurring at these times.
Depending on their location venous malformations may cause pain, swelling, restriction of movement or cosmetic issues. Occasionally the blood moves so slowly that the blood can clot within the malformation. Occasionally venous malformations can bleed especially if they are in a very superficial (near to the skin) position. Treatment may be necessary because of the appearance or for associated functional problems.
Typically the main symptoms include pain and swelling.
Typically the main symptoms include pain and swelling. giving a bluish discolouration and swelling. This can lead to cosmetic issues, depending on the site of the lesion.
Intermittently the venous malformation can become more acutely painful, swollen and hard. This is mainly due to acutely painful, swollen and hard. This is mainly due to These blood clots typically do not move to the lungs.
Sclerotherapy treatment involves the injection of a special chemical into the venous malformation to ultimately shrink it and relieve the symptoms it is causing. It is typically carried out as a day case procedure in hospital.
Various substances can be used but most commonly the chemical used is Sodium Tetradecyl sulphate (Fibrovein). When injected into a lesion it causes an inflammatory reaction which leads to localised blood clots and the formation of a scar in place of the venous malformation, causing the malformation to shrink.
Sclerotherapy is carried out under ultrasound and X-ray control. This allows the doctor needs to make sure that the needle goes into exactly the right place and to assess the degree of communication with veins nearby.
Often a ‘course’ of multiple injections are required to adequately treat a venous malformation and it can be some time before you notice a significant difference. Not all venous malformations are successfully treated in this way but in the vast majority of cases significant results are achieved.
Sclerotherapy is not a ‘cure’ for these malformations but is aimed at controlling symptoms and reducing the size. Sclerotherapy may not treat skin discolouration associated with some: malformations.
Treatment options are:
or a combination of these. If there are no symptoms then there is no need for treatment.
At first it important to determine the exact symptoms and to what degree this is distressing you or how much of an impact this is having on your life. The majority of venous malformations do not need treatment, but this can be reviewed at any time, especially if symptoms worsen or change. Venous malformations are not malignant and cannot become malignant (cancerous).
At first it important to determine the exact symptoms and to what degree this is distressing you or how much of an impact this is having on your life. The majority of venous malformations do not need treatment, but this can be reviewed at any time, especially if symptoms worsen or change. Venous malformations are not malignant and cannot become malignant (cancerous).
Treatment depends on the number of vascular spaces within the lesion and the amount of more solid tissue. Lesions with more spaces (i.e. more venous lakes) are more suitable for injection therapy or ‘sclerotherapy’ than those that are mostly solid in nature. Depending on the site, size and other factors certain lesions are suitable for surgical removal.
We wil discuss treatment options with you.
Varicose veins, or twisted and enlarged veins, can be treated with sclerotherapy. Varicose veins are usually in the legs. Spider veins, a mild form of varicose veins, can also be treated with sclerotherapy. Small varicose veins usually respond best to sclerotherapy.
Sclerotherapy involves injecting a solution into a vein with a needle. The sclerotherapy arrangement makes the vein scar. The scarring forces blood through healthier veins. The collapsed vein then fades.
Although treated veins may not disappear completely following sclerotherapy, they typically fade within a few weeks. The full results may not appear for up to a month.Some veins need more than one sclerotherapy treatment.
Sclerotherapy in mulund is generally finished to cause the veins to appear more appealing. The system additionally can further develop side effects connected with varicose veins, including:
Specialists recommend holding back to have sclerotherapy done after pregnancy or breastfeeding.
Sclerotherapy in mulund generally has few serious complications.
Side effects that can occur where the needle goes into the skin include:
These side effects usually go away within days to weeks. Some side effects may take months or longer to go away completely
Less-common side effects of sclerotherapy that might need treatment include:
Inflammation. This is normally gentle however may cause enlarging, warmth and inconvenience around the site where the needle went into the skin. It’s possible that taking a non-prescription painkiller will help. Ibuprofen and aspirin (Advil, Motrin IB, and others) are two examples.
clot of blood It may be necessary to drain a treated vein if a lump of clotted blood forms there. A condition known as deep vein thrombosis occurs when a blood clot can occasionally travel to a deeper vein in the leg.
A blood clot that travels from the leg to the lungs and blocks a vital artery is a risk of deep vein thrombosis. A pulmonary embolism is the medical term for this. Sclerotherapy in mulund related complications are extremely uncommon and require immediate medical attention. The side effects incorporate difficulty breathing, chest torment or tipsiness, or hacking up blood.
Bubbles of air. Minuscule air pockets can ascend in the blood. This may not result in symptoms. However, symptoms may include fainting, nausea, seeing light flashes, and headaches.
These side effects generally disappear. However, if you experience pain or difficulty moving your arms or legs following the procedure, contact your doctor.
Reaction to an allergen A hypersensitive response to the arrangement utilized for treatment is conceivable, however exceptional.
A physical examination is done by a healthcare provider prior to the procedure. The doctor looks at your veins and looks for problems with your blood vessels.
The provider asks questions about your medical history. Information needed about your medical history includes:
Recent illnesses or medical conditions, such as a heart condition or a history of blood clots.
The outcomes of any other treatments you’ve had for varicose veins.
You take medications or supplements, particularly aspirin, ibuprofen (such as Advil, Motrin IB, and others), naproxen sodium (such as Aleve, Anaprox DS), blood thinners, iron supplements, or herbal supplements.
Sclerotherapy in mulund is commonly finished in a medical care supplier’s office. It for the most part requires an hour or less to finish.
Sclerotherapy in mulund for spider veins or small varicose veins typically produces results within three to six weeks. Bigger veins could require 3 to 4 months. However, you may require more than one treatment to achieve your goals.
Veins that answer treatment for the most part don’t return. However, new veins may emerge.
The aorta is the largest vessel in your body and carries the blood away from your heart to the rest of your organs. A thoracic aneurysm occurs if the arterial wall below your rib cage weakens and develops a bulge, meaning blood is flowing into the weakened area.
The TEVAR procedure involves the placement of a covered stent (a metal mesh tube with a layer of fabric) into the weakened area of the artery. This provides a route for the blood to flow without pooling in the bulge.
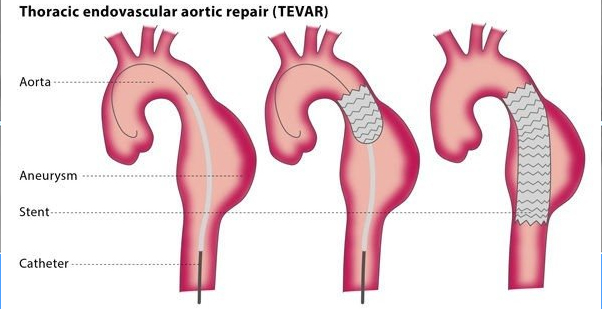
If the thoracic aneurysm was caused by trauma, such as if the patient was in an accident, TEVAR is a way to rapidly cover the injured area, controlling bleeding and preventing death.
Although surgical treatments for thoracic aortic aneurysms are available, surgery has a significantly higher risk of serious complications and death.
In most cases, the patient is given an epidural and a local anaesthetic for the procedure, although in some cases the patient is given a general anaesthetic.
The interventional radiologist will make a small cut in an artery at the top of your legs and will insert a sheath (a short tube to maintain safe access to the vessels). Then, the interventional radiologist will insert guidewires and catheters (thin flexible tubes) and direct them to the affected area under fluoroscopy. A contrast medium (dye) will be injected into the thoracic aorta so that the area clearly shows up under imaging for maximum accuracy. To place the stent, the interventional radiologist will insert it over a guidewire and move it to the correct location, where it will expand to seal the aneurysm or cover any leaks in the wall of the vessel.
After the procedure, your vital signs will be monitored and you will stay in hospital for 2-3 days. You may experience bruising and pain, though this can be treated with standard painkillers. Moving around once you are able to do so is encouraged. You will need to have the stent regularly checked using CT or ultrasound to ensure that the stent is in good condition and to avoid long-term problems.
Thoracic duct embolization (TDE) is a percutaneous, image-guided occlusion of the TD. This technique was devised by one of the pioneers of Interventional Radiology, Dr Constantine Copez. Originally envisioned as a minimally invasive alternative to TD ligation, it is a 3-step process consisting of lymphangiography followed by percutaneous transabdominal catheterization of the CC and embolization of the TD proximal to the leak or occlusion. Embolization is most commonly a combination of coils and n-butyl cyanoacrylate (n-BCA) Lymphangiography historically was a time-consuming and technically challenging pedal cut down. There has been an update to the procedure with inguinal intranodal lymphangiography. This recent adaptation has made the procedure considerably shorter.In patients in whom percutaneous CC cannulation fails, the TD may be accessed from a retrograde approach from the subclavian vein.
A venogram is a test that lets your healthcare provider see the veins in your body, especially in your legs. A special dye is injected that can be seen on an special X-ray in cath-lab . The dye lets your healthcare provider see your veins and how healthy they are.
A venogram is used to diagnose deep vein thrombosis (DVT) or other abnormalities of your veins. This test can also help your healthcare provider diagnose other health problems.
Venous recanalization is performed by a specially trained interventional radiologist. By placing small tubes in the vein and using specialized equipment for image guided procedures, the closed off SVC can be reopened with a balloon. When necessary a special metal stent can be placed to keep the vein open.

A phlebectomy in mulund is a minimally invasive procedure for removing varicose veins that lie just beneath the surface of the skin.
Previously, surgical removal (known as “vein stripping”) was the only effective method of treating varicose veins. The procedure involved significant discomfort and recovery time. Fortunately, a phlebectomy is a less invasive method of treating varicose veins, along with the pain that may be associated with the condition.
Varicose veins that are just below the surface of the skin can be removed with a minimally invasive procedure known as a phlebectomy.
The only effective treatment for varicose veins in the past was surgical removal, or “vein stripping.” The procedure was painful, and it took some time to recover. Fortunately, a phlebectomy in mulund is a less invasive treatment for varicose veins and the possible pain they cause.
A phlebectomy in mulund is a procedure that removes varicose veins just below the surface of the skin with a small scalpel or needle. It is minimally invasive. The system is additionally called Wandering Phlebectomy, Microphlebectomy, and Cut Separation.
The varicose vein is removed piece by piece through a series of tiny cuts in the skin, which are also known as “stab incisions.” Most of the time, the incisions are so small that no stitches are needed.
A local anesthetic is used during the procedure, which is carried out at the Mulund pain clinic. Varicose veins of any size can be safely and effectively treated with a phlebectomy in mulund.
There is little discomfort and no downtime during the procedure; As a result, the patient is able to stand up and walk after the procedure. Ordinarily, a patient can continue a normal everyday schedule the following day.
In order to speed up the healing process, the doctor may order the patient to wear a compression stocking or bandage for at least a week. Additionally, the procedure may result in brief bruising and swelling.
Following treatment, the majority of patients will not require any prescription pain medication. Ice packs and prescription painkillers are sufficient for most conditions. The majority of patients return to work and normal activities the following day, so downtime is also minimal.
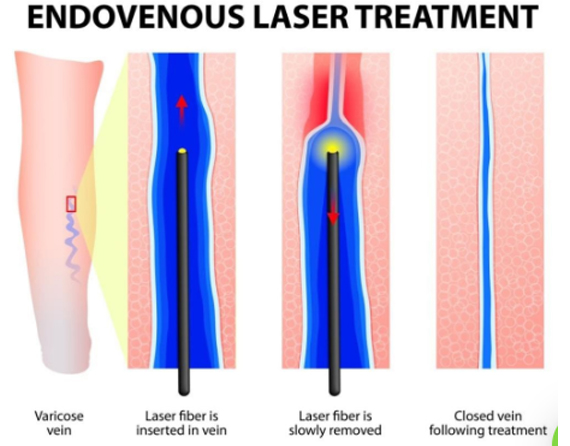
Frequently, a phlebectomy in mulund is utilized related to other normal vein evacuation methodology like endovenous laser treatment (EVLT) and sclerotherapy to address distinctively measured veins and to yield the best superficial outcomes.
Local anesthesia is administered along the vein after the veins that need to be removed have been identified. After that, the doctor makes a few small cuts to separate the vein into sections. A little snare tenderly eliminates the segments of the vein. Eliminating the vein in segments limits the event of blood clusters and empowers quicker recuperating.
After the procedure is finished, the incisions are covered with a dressing, and the leg is wrapped in a compression wrap that is snug but comfortable. To reduce the likelihood of a blood clot, the patient is asked to walk around for 10 to 15 minutes before leaving the office. Gradual compression stockings are also required for patients, which aid in healing.
The long-term success rate of a phlebectomy is 90%. Varicose veins diminish noticeably after the initial bruising subsides. In comparison to other procedures, a phlebectomy in mulund has the following additional advantages:
The incisions (cuts) may cause some mild pain on the day of surgery. If you have any pain, take nonsteroidal anti-inflammatory drugs (NSAIDs) that you can buy over the counter. Converse with your supplier about some other prescriptions you take and adhere to their directions on any progressions to your medicine.
The specialist will put Pro wraps and dressing on your leg after medical procedure. They will likewise give you pressure stockings to bring back home. The day after surgery, you can remove the bandages, but you will need to wear compression stockings for two to three weeks while your leg heals.
For one to two weeks after surgery, you may experience:
Use NSAID pain medication and an ice pack to relieve pain and soreness. You can also elevate your leg above your heart for further pain relief and to reduce bleeding.
Phlebectomy in mulund procedures are safe, but they do come with some risks, such as: