
Neurology focuses on conditions affecting the brain, spine, and nervous system, which control essential body functions. Disorders such as stroke, aneurysms, vascular malformations, and nerve-related issues require timely diagnosis and precise treatment to prevent long-term complications.
Dr. Ravi Manek provides advanced, minimally invasive, image-guided neurological interventions to treat complex neurovascular conditions with high accuracy. These procedures help restore blood flow, reduce risks, and improve overall neurological function without the need for major surgery.
With a focus on safety and patient care, treatments are tailored to each individual, ensuring faster recovery, minimal discomfort, and better long-term outcomes for neurological health.
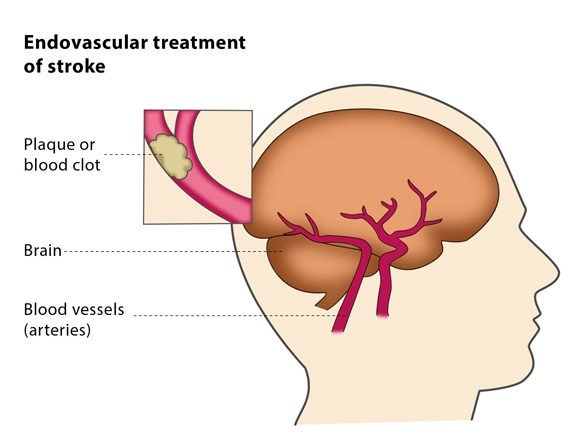
What is an endovascular treatment of stroke?
Endovascular treatment of stroke is the non-surgical treatment for the sudden loss of brain function due to blood clots. The treatment uses microcatheters (thin tubes visible under X-rays) which are inserted into the blood clot from the groin or the arm. The blood clot is removed from the blood vessel – this procedure is called a thrombectomy. If the blood clot cannot be removed, it is liquefied using drugs delivered through the catheter, in a procedure known as thrombolysis.
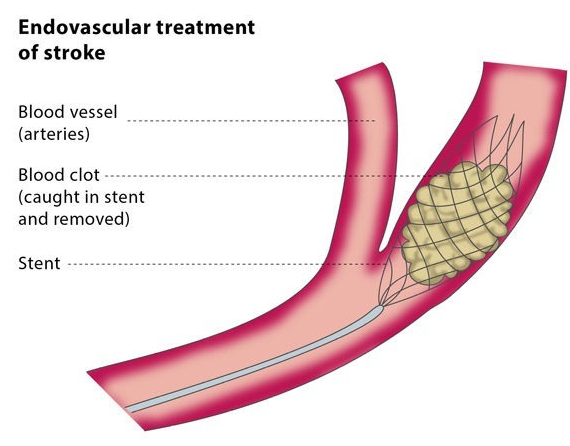
The interventional radiologist will insert a catheter into an artery in your arm or groin and move it towards the blood clot under X-ray guidance. The blood clot is removed in a procedure called a thrombectomy. The blood clot may be removed by trapping it in a stent which is then pulled out with the clot, or the interventional radiologist may suck the clot out through the catheter.
If the clot cannot be removed, a medication may be applied through the catheter to liquefy it. If the blood vessel is too narrow, a balloon catheter can be used to restore its original size, in a procedure called an angioplasty. Afterwards, a stent is inserted to hold the blood vessel open.
If you have suffered stroke caused by a blockage in a large artery but you are not suitable for or have not responded to thrombolysis, this procedure is a possible treatment for you.
The insertion of catheters and guidewires in arteries to the brain carries a low but definite risk of bleeding or the movement of blood clots to previously unaffected parts of the brain. Endovascular treatment is inadvisable if your admission to hospital after the stroke was delayed, as this carries a higher risk of complications.
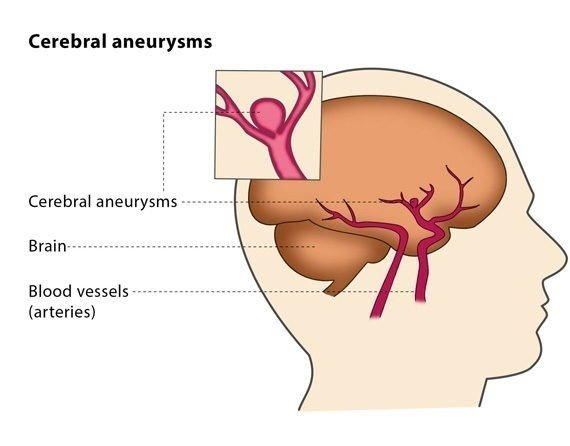
What is endovascular treatment of intracranial aneurysms?
An aneurysm is a weakness in the wall of a blood vessel which causes the blood vessel to swell. When an aneurysm develops inside the brain, it is called an intracranial aneurysm. Intracranial aneurysms are associated with a high risk of bleeding in and around the brain, which can have catastrophic consequences. Endovascular treatment of intracranial aneurysms is the non-surgical treatment of intracranial aneurysms using microcatheters (small and flexible plastic tubes) and X-ray guidance.
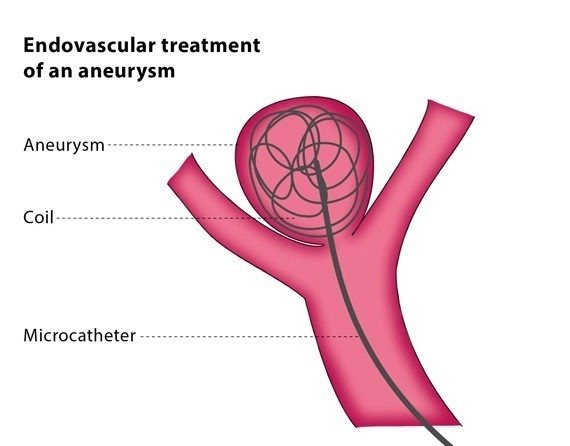
The procedure involves inserting tiny metal spirals (coils) into the blood vessel to act as a physical barrier and encourage blood clotting, preventing bleeding. A metal mesh tube (stent) may be used to keep the coils in place and support the walls of the blood vessel. Sometimes stents are used without coils to change the blood flow and encourage clotting in the aneurysm.
You will be under general anaesthesia for the procedure. Using fluoroscopy for guidance, the interventional radiologist will insert a catheter through an artery in your groin or arm and will move it to the location of the aneurysm.
The interventional radiologist will then deposit tiny metal coils through the catheter and into the aneurysm, which stimulate blood clotting. Filling the aneurysm in this way stops blood flow to this area. A stent may be used to hold the coils in place and cover the aneurysm.
A ruptured intracranial aneurysm that causes bleeding to the brain or to the surface of the brain should be treated urgently to stop the bleeding, minimise damage to the brain and prevent bleeding in the future. Unruptured aneurysms are sometimes treated to minimise any future risk.
The procedure carries a risk of the aneurysm bursting, leading to bleeding in and around the brain. One or more of the coils may move out of place in the aneurysm or blood clots may develop during or after the procedure, either of which may block important blood vessels. You will probably be prescribed treatment to prevent blood clots developing for at least three months.
Provides an image of the blood vessels in the brain to detect a problem with blood flow. The procedure involves inserting a catheter (a small, thin tube) into an artery in the leg and passing it up to the blood vessels in the brain. A contrast dye is injected through the catheter and X-ray images are taken in Cath Lab of the blood vessels.
In a patient with Subarachnoid Haemorrhage, between 3rd to 15th days of haemorrhage; there is chances of arterial narrowing called vasospasm.
Due to Vasospasm, patient may have transient ischemic attacks or stroke. These patients are treated with intra-arterial Nimodipine & Milrinoneinfusion. To dilate arteries chemical (drug) is infused so this process is called as chemical angioplasty.
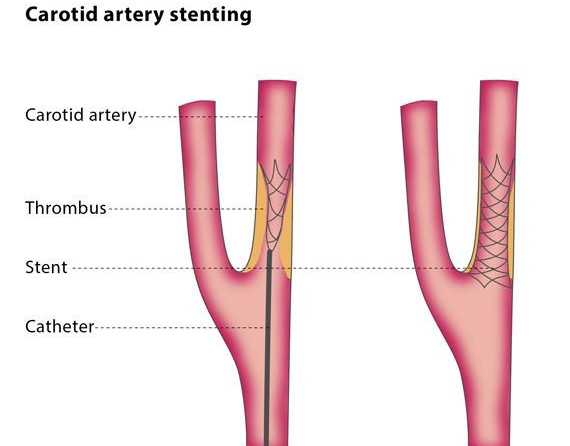
The carotid arteries are the two large arteries on each side of your neck that supply your brain, neck and face with oxygenated blood. Sometimes plaque builds up in the arteries, which results in a condition called carotid artery stenosis (also known as carotid artery disease). Stenosis means that the space inside the artery has narrowed, restricting blood flow.
Carotid artery stenting (CAS, also referred to as carotid artery angioplasty with stenting) is a minimally invasive treatment option for effectively managing carotid artery stenosis and preventing stroke. It is a non-surgical treatment in which catheters (thin hollow tubes) are used to place a stent (a metal mesh tube) in the affected artery to ensure the passage stays clear, thus restoring blood flow.
While some patients with carotid artery stenosis have no symptoms, the condition can lead to the formation of blood clots (thrombosis), mini-strokes (which are similar to strokes but only last a few minutes) and strokes (where the artery supplying blood to the brain is blocked). The CAS procedure is a possible alternative for patients for whom the traditional surgical option, carotid endarterectomy (CEA), may not be suitable.
You will be given a local anaesthetic for the procedure. Using fluoroscopy to monitor and guide the process, the interventional radiologist will puncture an artery in your groin or arm with a needle, and will insert a balloon-tipped catheter into the carotid artery, guiding the catheter into the narrowed area. The balloon will then be inflated and deflated, compressing the fatty plaque or blockage against the artery walls, widening the blood vessel and increasing blood flow. After this, the balloon will be removed.
The interventional radiologist will use another catheter to place a stent, and, in some cases, will further expand the stent using another balloon-tipped catheter. The stent remains in place so that there is a clear passage in your artery.
CAS may be an appropriate treatment for you if you have symptoms of carotid artery disease and are at increased risk of suffering complications from surgery. It may be beneficial if you have undergone traditional surgery but your arteries have become re-narrowed (called restenosis), if the location of the narrowing in the artery means it cannot be operated on or if narrowing has occurred following radiation treatment. It may also be considered as a treatment for you if you have no symptoms of carotid artery disease but are awaiting surgery for carotid stenosis.
Carotid paragangliomas, commonly referred as carotid body tumors (CBTs), are the most common neuroendocrine tumors in the head and neck. They are most commonly located at the bifurcation of the common carotid artery and usually present as a painless neck mass.
Carotid body tumour are highly vascularized tumors which can make tumor resection particularly challenging. Specifically, vascular and neurologic sequelae are feared complications of CBT surgical therapy. Schick et al. first introduced the concept of preoperative embolization in 1980 and reported the first such CBT resection. Since then, several studies have evaluated the impact of preoperative embolization on CBT surgery. There is evidence suggesting that preoperative selective embolization may reduce blood loss during surgery and decrease the risk of perioperative complications
The aim of the procedure is to stop the blood flowing into the vessels which supplies the CTB.
The interventional radiologist will insert a 2-3 mm tube into your groin and then guide the tube under imaging to the blood vessel suppling the CTB . They will then insert small resin particles (known as microparticles) into the vessels. This causes the vessel or vessels to become blocked and so stops the bleeding.
Carotid paragangliomas, commonly referred as carotid body tumors (CBTs), are the most common neuroendocrine tumors in the head and neck. They are most commonly located at the bifurcation of the common carotid artery and usually present as a painless neck mass.
Carotid body tumour are highly vascularized tumors which can make tumor resection particularly challenging. Specifically, vascular and neurologic sequelae are feared complications of CBT surgical therapy. Schick et al. first introduced the concept of preoperative embolization in 1980 and reported the first such CBT resection. Since then, several studies have evaluated the impact of preoperative embolization on CBT surgery. There is evidence suggesting that preoperative selective embolization may reduce blood loss during surgery and decrease the risk of perioperative complications.
The aim of the procedure is to stop the blood flowing into the vessels which supplies the CTB.
The interventional radiologist will insert a 2-3 mm tube into your groin and then guide the tube under imaging to the blood vessel suppling the CTB . They will then insert small resin particles (known as microparticles) into the vessels. This causes the vessel or vessels to become blocked and so stops the bleeding.
he treatment of skull base lesions such as tumors, aneurysms, and traumatic lesions may require internal carotid artery (ICA) sacrifice. Pretherapeutic knowledge of carotid artery dependence is essential in these patients, since vascular bypass or alternative surgical approaches may be necessary in those unable to tolerate ICA sacrifice. Balloon test occlusion (BTO) is an angiographic test to evaluate ischemic tolerance after permanent occlusion of an ICA. During BTO, the cerebral hemisphere ipsilateral to the tested ICA may be perfused by collateral blood flow, depending on the development of collateral pathways including the circle of Willis (COW).
Cushing’s syndrome is a result of hypercortisolism, which can be due to excessive corticotropin (ACTH) secretion from a pituitary or nonpituitary ACTH-secreting tumor, which drives adrenal cortisol production (ACTH-dependent), or by autonomous adrenal secretion of excessive amounts of cortisol, which is not stimulated by ACTH (ACTH-independent). Identifying the source of ACTH in ACTH dependent Cushing’s is the key to its management. Although Magnetic Resonance Imaging (MRI) is the next investigation of choice, it has lower sensitivity and specificity, and microadenomas that secrete ACTH may be too small to be detected with MRI[. Inferior petrosal sinus sampling (IPSS) is the most reliable method in the confirmation of a central cause of Cushing’s syndrome.
You will be given a local anaesthetic for the procedure. Using fluoroscopy to monitor and guide the process, the interventional radiologist will puncture an artery in your groin or arm with a needle, and will insert a small catheter in the brain and take few samples of blood from Inferior Petrosal Sinus and send for processing.
Epistaxis is the medical term for a nosebleed, which is relatively common and refers to bleeding from the nose. A nosebleed may be caused by a number of things, including blunt trauma, infections, tumours and the structure of your nose.
Epistaxis embolisation is a minimally invasive procedure in which the blood vessel is deliberately blocked in order to stop the nosebleed.
The aim of the procedure is to stop the blood flowing into the vessels which cause the nosebleed, without preventing blood from flowing into the area around the affected vessel.
The interventional radiologist will insert a 2-3 mm tube into your groin and then guide the tube under imaging to the blood vessel causing the nosebleed. They will then insert small resin particles (known as microparticles) or small metal spirals (coils) into the bleeding vessel or vessels. This causes the vessel or vessels to become blocked and so stops the bleeding.
The main reason to treat nosebleeds is the risk of breathing in blood, as if too much blood is inhaled there is a risk of death.
Intracranial( inside the brain) atherosclerotic diseas/stenosis (ICAD) is considered a major cause of recurrent cerebrovascular events. ICAD continues to be a disease without an effective method of reducing the risk of recurrent stroke and death, even with aggressive, highly monitored medical treatment.
Stenosis means that the space inside the artery has narrowed, restricting blood flow
Intra cranial stenting is a minimally invasive treatment option for effectively managing intra cranial stenosis and preventing stroke. It is a non-surgical treatment in which catheters (thin hollow tubes) are used to place a stent (a metal mesh tube) in the affected artery to ensure the passage stays clear, thus restoring blood flow.