
Obstetrics & Gynecology focuses on women’s reproductive health, pregnancy care, and hormonal wellness. These specialties address a wide range of conditions involving the uterus, ovaries, fallopian tubes, and overall reproductive system, ensuring women receive comprehensive support at every stage of life.
Through advanced, image-guided procedures, many gynecological issues such as fibroids, cysts, abnormal bleeding, and pelvic pain can be treated with precision and minimal discomfort. These minimally invasive techniques offer safer alternatives to traditional surgery, helping patients recover faster and return to daily activities sooner.
With a holistic and patient-first approach, care is tailored to promote long-term reproductive health, comfort, and overall well-being. Whether managing complex conditions or offering supportive care during pregnancy, the focus is on safety, accuracy, and compassionate treatment.
UFE or uterine Fibroid embolisation is a relatively new procedure in which the blood supply to the fibroids is blocked off causing the fibroids to shrink.
This treatment is carried out by an interventional radiologist rather than a gynaecologist.
Fibroids are non-cancerous growth, usually found in the uterus of women in their childbearing age.
These fibroids can be more than one and grow in size, with time. While they may be asymptomatic, depending on the size and location of the fibroid in the uterus.
Uterine Fibroid Embolisation (UFE), also called as Uterine Artery Embolisation is a minimally invasive procedure done under local anaesthesia, using fluoroscopy guidance.
An Interventional Radiologist inserts a thin catheter inside a thigh artery and guides it to the uterine artery. Tiny round particles called PVA (Poly Vinyl Alcohol) are injected into the blood vessels of the uterine artery for embolisation.
These particles block blood flow to the fibroids, causing them to shrink. The PVA particles remain permanently at the fibroid site.
After a uterine fibroid/artery embolization, there is immediate relief from heavy bleeding. Pressure / size related symptoms take about a few weeks or months to disappear.
Since the uterine artery embolization cuts off blood and necessary nutrients for fibroid growth, they gradually shrink over a period of 3 – 6 months. Once the fibroids have shrunk, they do not grow back.
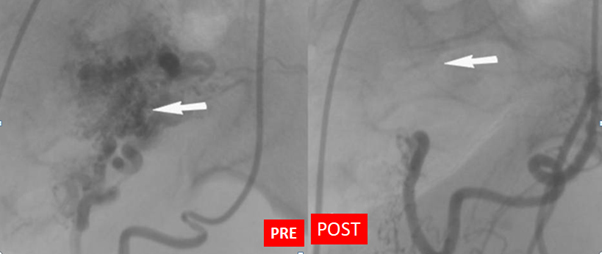
Uterine arteriovenous malformation (AVM) is a rare but potentially life-threatening source of bleeding. AVMs have been reported in patients from 18 to 72 years old. Uterine AVMs are characterized by multiple communications of varying sizes between arteries and veins in the same vicinity.
Traditionally, hysterectomy or uterine arteries ligation were the treatment modalities for cases of uterine AVMs. Angiographic arterial embolization has recently become the preferred management protocol because it is minimally invasive and has the potential to preserve fertility.
An atypical embolization procedure is as follows: Using the Seldinger technique through the common femoral artery, initial pelvic angiography is performed followed by selective internal iliac angiography and uterine angiography on the side presumed to be affected during ultrasonographic examination. Embolic materials are carefully introduced into the uterine artery or other feeding arteries until stasis of flow is confirmed angiographically.
Pelvic venous congestion syndrome is also known as ovarian vein refluxcaused by dilatation of the ovarian and/or pelvic veins.
Pelvic pain or aching around the pelvis and lower abdomen
Dragging sensation or pain in the pelvis
Feeling of fullness in the legs
Worsening of stress incontinence
Worsening in the symptoms associated with irritable bowel syndrome
The usual treatment is percutaneous transcatheter pelvic vein embolisation.
The usual treatment is percutaneous transcatheter pelvic vein embolisation.
Pelvic vein embolisation is a minimally invasive procedure performed by a specially trained interventional radiologist in the interventional radiology suite.
Using x-ray image guidance and contrast material to see the blood vessels, the catheter is then directed into abnormal ovarian and/or pelvic vein.
Abnormal vein is sealed and blocked using synthetic material or medication called embolic agents.
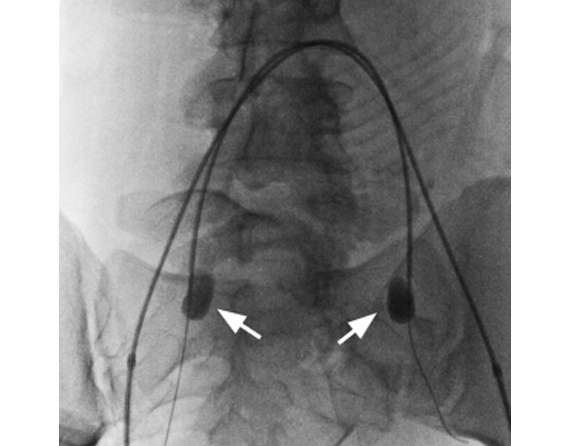
The term placenta accreta spectrum disorder (PASD) is used to describe the morbidly adherent placenta, which includes placenta accreta, increta, and percreta. In past decades, women increasingly preferred to deliver by cesarean section (CS), leading to the increasing incidence of placenta accrete spectrum (PAS). It is reported with an incidence of 1 per 533 pregnancies. One of the main and deadliest complications of PAS is massive bleeding. the average blood loss in these cases has been estimated to range between 2 and 3 liters. Additionally, the morbidly adherent placenta is the most common indication for peripartum hysterectomy, which is associated with high rates of morbidity and mortality. Therefore, strategies to prevent and treat bleeding are therefore critical. Various approaches have been employed in controlling intraoperative blood loss in cases of abnormal placentation, including inserting uterine tamponade balloons, applying uterine gauze packing, placing uterine brace or isthmic compression sutures, and performing a hysterectomy. The arterial occlusion balloon has been used in PAS recently, and the role of internal iliac artery (IIA) balloon occlusion to improve hemorrhagic outcomes in women with placenta accreta has been evaluated in many studies, which showed beneficially.
Postpartum hemorrhage (PPH) is a serious complication of giving birth that can result in death. Interventional radiology allows for the use of uterine artery embolization and transcatheter arterial embolization to prevent and treat PPH. These procedures are minimally invasive options that use the uterine or internal iliac arteries to place either a balloon or embolic material to stop the bleeding.
Fallopian tube recanalization (FTR) is a nonsurgical procedure to clear blockages in the fallopian tubes, part of a woman’s reproductive system.
A common cause of female infertility is a blockage of the fallopian tubes, usually as the result of debris that has built up.
Occasionally, scarring from surgery or serious infection can lead to a blockage as well.
Fallopian tube recanalization (FTR) is a minimally invasive procedure done by interventional radiologists use to treat these blockages.
Recanalization is the medical term for “reopening.”
No cut / No suture procedure.
Varicose veins in pregnancy are twisted and bulgy veins that protrude on the surface of the skin. Spider veins are similar, but less obvious. These blue and red tattoo like lines on the skin, as well as the varicose veins are commonly found in the legs and occur primarily due to enlarged and weakened vein walls and faulty valves. This leads to a painful and problematic condition that sometimes necessitates spider/varicose vein treatment. Vascular defects and poor blood circulation are also important reasons for these vein disorders.
Varicose vein laser surgery involves applying a highly concentrated beam of light (laser) to the inner lining of vein with extreme precision, not affecting the surrounding tissue. The laser energy heats the inner lining of the swollen varicose veins in leg, causing it to shrink and collapse. The body automatically and safely reroutes the blood through other healthy veins.
Like all other successful laser treatments, EVLT Varicose vein treatment is also very successful as well as safe. EVLT (laser) varicose vein treatment has a 98% initial success rate with excellent long term results.